

Regression of Multiple Intracranial Meningiomas With Cessation of Progesterone Agonist Therapy: A Case Report
- PMID: 38371126
- PMCID: PMC10873817
- DOI: 10.7759/cureus.52479
Regression of Multiple Intracranial Meningiomas With Cessation of Progesterone Agonist Therapy: A Case Report
Abstract
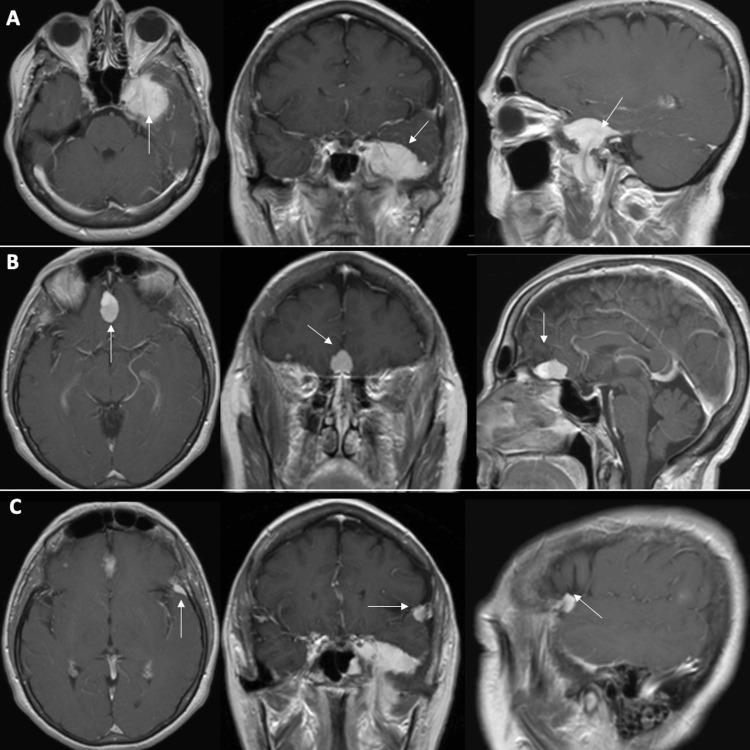
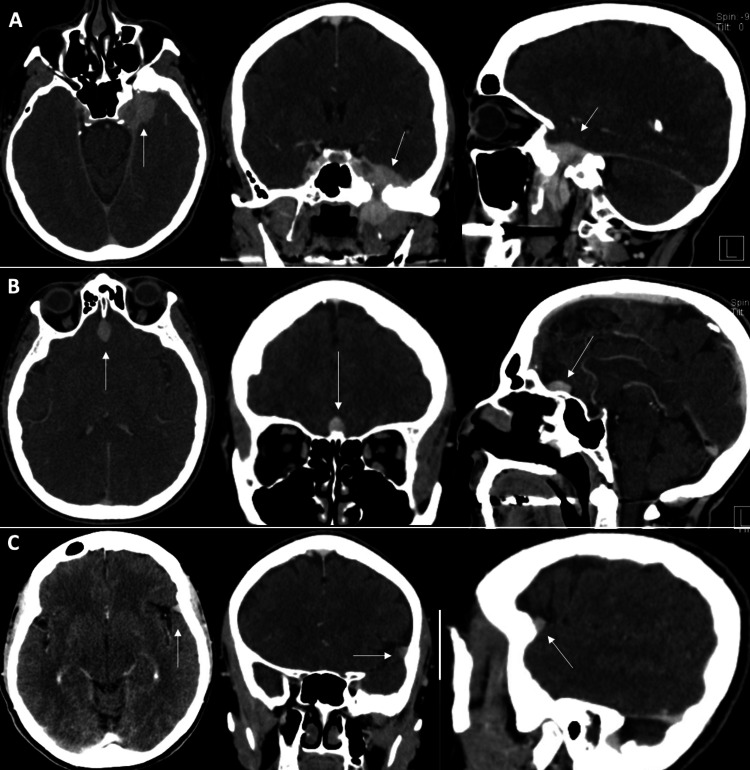
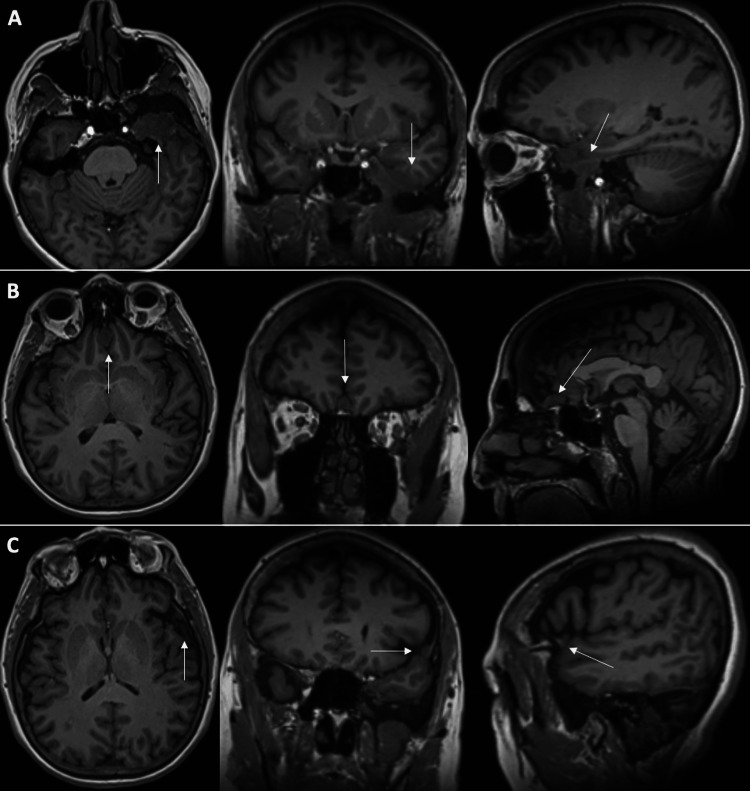
In this case report, we discuss a patient who experienced spontaneous regression of multiple intracranial meningiomas that were treated conservatively for 5 years after cessation of megestrol acetate, an exogenous progestin. In addition, we discuss the previous literature describing the relationship between exogenous progesterone medications and meningioma growth. This case, along with others reported, implies that cessation of progesterone therapy, when feasible, may alter the natural history of meningioma growth and thus impact treatment decisions.
Keywords: extra-axial lesion; hormonal influence on meningioma; megestrol acetate; meningioma; progestin.
Copyright © 2024, Bailey et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Intracranial meningiomas in patients with uterine sarcoma treated with long-term megestrol acetate therapy.World Neurosurg. 2011 Nov;76(5):477.e16-20. doi: 10.1016/j.wneu.2011.03.035. World Neurosurg. 2011. PMID: 22152580
-
Regression of multiple intracranial meningiomas after cessation of long-term progesterone agonist therapy.J Neurosurg. 2010 May;112(5):920-4. doi: 10.3171/2009.8.JNS09201. J Neurosurg. 2010. PMID: 19731987
-
Regression of multiple intracranial meningiomas after cessation of long-term synthetic progesterone (megestrol) medication: case report and autopsy.Free Neuropathol. 2024 Oct 29;5:27. doi: 10.17879/freeneuropathology-2024-5813. eCollection 2024 Jan. Free Neuropathol. 2024. PMID: 39473896 Free PMC article.
-
Estrogen and Progesterone Therapy and Meningiomas.Endocrinology. 2022 Feb 1;163(2):bqab259. doi: 10.1210/endocr/bqab259. Endocrinology. 2022. PMID: 34935947 Review.
-
Secondary intracranial meningiomas after high-dose cranial irradiation: report of five cases and review of the literature.Int J Radiat Oncol Biol Phys. 2000 Aug 1;48(1):65-73. doi: 10.1016/s0360-3016(00)00609-x. Int J Radiat Oncol Biol Phys. 2000. PMID: 10924973 Review.
Cited by
-
Spontaneous regression of a petroclival meningioma: illustrative case.J Neurosurg Case Lessons. 2024 Oct 7;8(15):CASE24416. doi: 10.3171/CASE24416. Print 2024 Oct 7. J Neurosurg Case Lessons. 2024. PMID: 39378522 Free PMC article.
References
-
- Meningiomas arising from the tuberculum sellae: with the syndrome of primary optic atrophy and bitemporal field defects combined with a normal sella turcica in a middle-aged person. Cushing H, Eisenhardt L. JAMA Ophthalmol. 1929;1:1.
-
- Estrogen and progesterone therapy and meningiomas. Hage M, Plesa O, Lemaire I, Raffin Sanson ML. Endocrinology. 2022;163 - PubMed
-
- Estrogen and progesterone receptors in meningiomas. Maiuri F, Montagnani S, Gallicchio B. Surg Neurol. 1986;26:435–440. - PubMed
-
- Growth of a meningioma in a transsexual patient after estrogen-progestin therapy. Gazzeri R, Galarza M, Gazzeri G. N Engl J Med. 2007;357:2411–2412. - PubMed
Publication types
LinkOut - more resources
Full Text Sources