

Transperineal drainage of prostate abscesses: A minimally invasive, low-risk management strategy that yields satisfactory results
- PMID: 38371211
- PMCID: PMC10869666
- DOI: 10.1002/bco2.310
Transperineal drainage of prostate abscesses: A minimally invasive, low-risk management strategy that yields satisfactory results
Abstract
Objectives: In this narrative review, we aim to present two cases of transperineal drainage of prostate abscesses with a good clinical outcome. Furthermore, we reviewed the literature on this treatment approach and aim to propose a minimally invasive protocol for managing this rare condition.
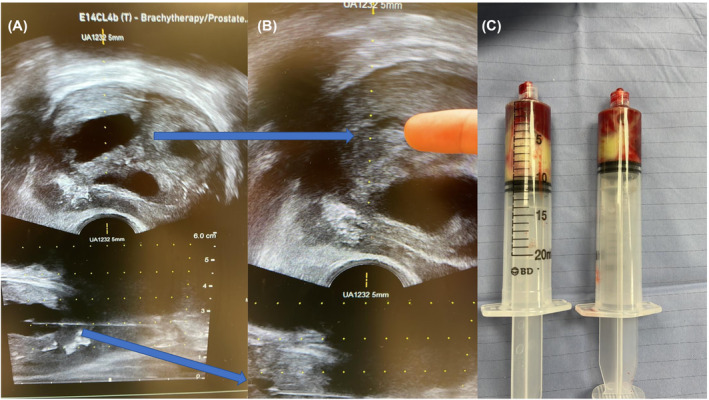
Patients and methods: Our patients are 33- and 61-year-old males who both underwent uncomplicated transperineal drainage of prostate abscess with the use of a Precision Point device with rapid clinical improvement and complete resolution of the abscess within the follow-up period. We used PubMed to conduct a literature search and included and evaluated 16 relevant case reports and case series in which the authors utilized transperineal drainage techniques for prostatic abscesses.
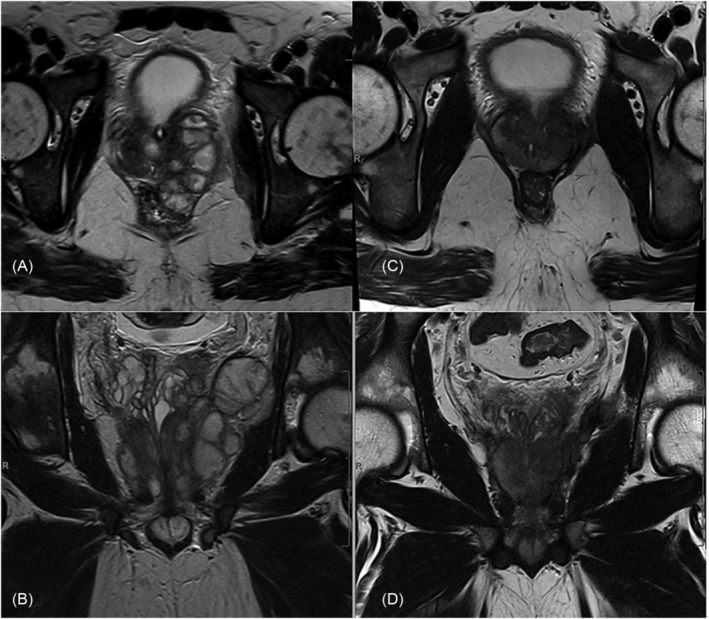
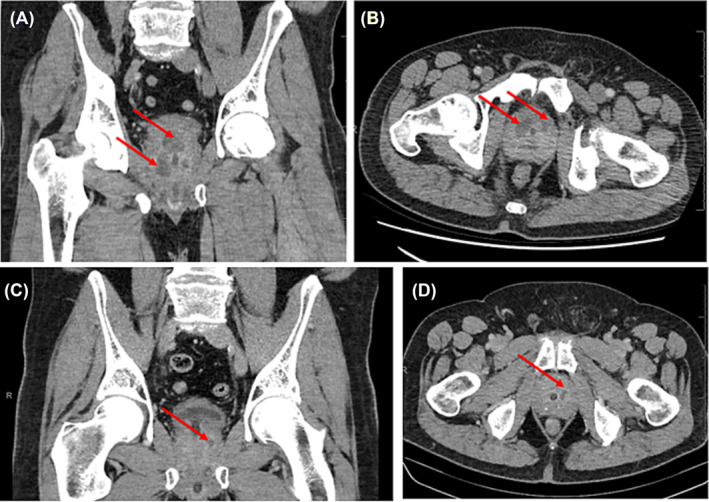
Results: Our first patient was young and very unwell with sepsis and a pulmonary embolism. He had a complex abscess extending through the prostate to the left pelvic side wall. Trans-gluteal drainage of the pelvic side-wall collection was required in addition to transperineal drainage of the prostate abscess. After drainage and a prolonged course of antibiotics, he achieved resolution of the abscess by 7 weeks with ejaculatory function intact. Our second patient who was very keen on the preservation of ejaculatory function had multiple small abscesses and underwent transperineal drainage. He had significant interval improvement of his abscess burden at the 4-week follow-up and complete resolution at the 6-month follow-up. The total number of cases in the literature on our review is 22, with considerable variability in how the authors managed the prostate abscesses that underwent transperineal drainage, including variability in their follow-up time frame, choice of imaging modality, duration of antibiotic treatment, drain placement, and use of irrigation solutions (including antibiotics) into the abscess cavity. Furthermore, the sizes of the prostate abscesses were not consistently reported. Given the small sample size and variability in management from different authors, it was not possible to draw any statistical analysis.
Conclusion: Transperineal prostate abscess drainage combined with prolonged antibiotic therapy provides a less invasive alternative to treating prostate abscesses for those who which to preserve ejaculatory function and avoid the other adverse events of transurethral de-roofing. In itself, it can achieve complete resolution of abscess. It provides the benefit of drainage under real-time imaging; for percutaneous drain placement; prevents urethral injury; retrograde ejaculation; and can be done under local anaesthetic which is preferable for the unstable patient. The utility of the procedure may be limited by the complexity of the abscess or whether it has extended beyond the prostate. The patient should always be informed that further drainage via percutaneous methods or transurethral methods may be necessary if their clinical condition does not improve. We recommend this procedure be offered as an alternative to transurethral methods in younger patients and those who would like to preserve ejaculatory function. Furthermore, we highly encourage a prolonged course of antibiotic therapy and interval follow-up with clinical review of symptoms and imaging to confirm resolution.
Keywords: TRUS; infection; prostate abscess; transperineal; transperineal drainage.
© 2023 The Authors. BJUI Compass published by John Wiley & Sons Ltd on behalf of BJU International Company.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Simultaneous prostatic and right seminal vesicle abscesses: a case report.J Med Case Rep. 2024 Nov 8;18(1):543. doi: 10.1186/s13256-024-04896-3. J Med Case Rep. 2024. PMID: 39516892 Free PMC article.
-
Three-dimensional ultrasound guidance for percutaneous drainage of prostatic abscesses.Urology. 2004 Jun;63(6):1017-20; discussion 1020. doi: 10.1016/j.urology.2003.12.040. Urology. 2004. PMID: 15183937
-
[Prostatic abscess--diagnosis and treatment].Harefuah. 2008 Jul;147(7):594-6, 663. Harefuah. 2008. PMID: 18814516 Hebrew.
-
Transurethral microwave thermotherapy for the treatment of lower urinary tract symptoms in men with benign prostatic hyperplasia.Cochrane Database Syst Rev. 2021 Jun 28;6(6):CD004135. doi: 10.1002/14651858.CD004135.pub4. Cochrane Database Syst Rev. 2021. PMID: 34180047 Free PMC article.
-
Diagnosis and management of complications following pelvic organ prolapse surgery using a synthetic mesh: French national guidelines for clinical practice.Eur J Obstet Gynecol Reprod Biol. 2024 Mar;294:170-179. doi: 10.1016/j.ejogrb.2024.01.015. Epub 2024 Jan 17. Eur J Obstet Gynecol Reprod Biol. 2024. PMID: 38280271 Review.
Cited by
-
A rare case report of severe prostate abscess treated with artificial intelligence-assisted mpMRI-TRUS real-time-guided puncture drainage.SAGE Open Med Case Rep. 2024 Nov 20;12:2050313X241301860. doi: 10.1177/2050313X241301860. eCollection 2024. SAGE Open Med Case Rep. 2024. PMID: 39574497 Free PMC article.
-
A Rare Case of Prostate Abscess With Pyelonephritis in an Adolescent Male.Cureus. 2025 Jul 5;17(7):e87345. doi: 10.7759/cureus.87345. eCollection 2025 Jul. Cureus. 2025. PMID: 40761953 Free PMC article.
-
Emphysematous Prostatic Abscess: A Case Report and Literature Review.Clin Case Rep. 2025 Jun 4;13(6):e70544. doi: 10.1002/ccr3.70544. eCollection 2025 Jun. Clin Case Rep. 2025. PMID: 40475351 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources