

Eomesodermin-expressing CD4+ Th cells and association with pregnancy in multiple sclerosis
- PMID: 38371384
- PMCID: PMC10874138
- DOI: 10.1177/17562864241229321
Eomesodermin-expressing CD4+ Th cells and association with pregnancy in multiple sclerosis
Abstract
Background: Pregnancy in patients with multiple sclerosis (MS) is accompanied by a decline of relapse activity with increased risk of relapses 3 months post-partum, for unknown reasons. Eomesodermin+ T-helper cells (Eomes+ Th cells) are known to mediate neuroinflammation and disease progression in MS and are induced by prolactin-secreting cells.
Objectives: Here, investigated immune cell alterations and the pathophysiological role of Eomes+ Th cells for disease activity during pregnancy and post-partum in MS.
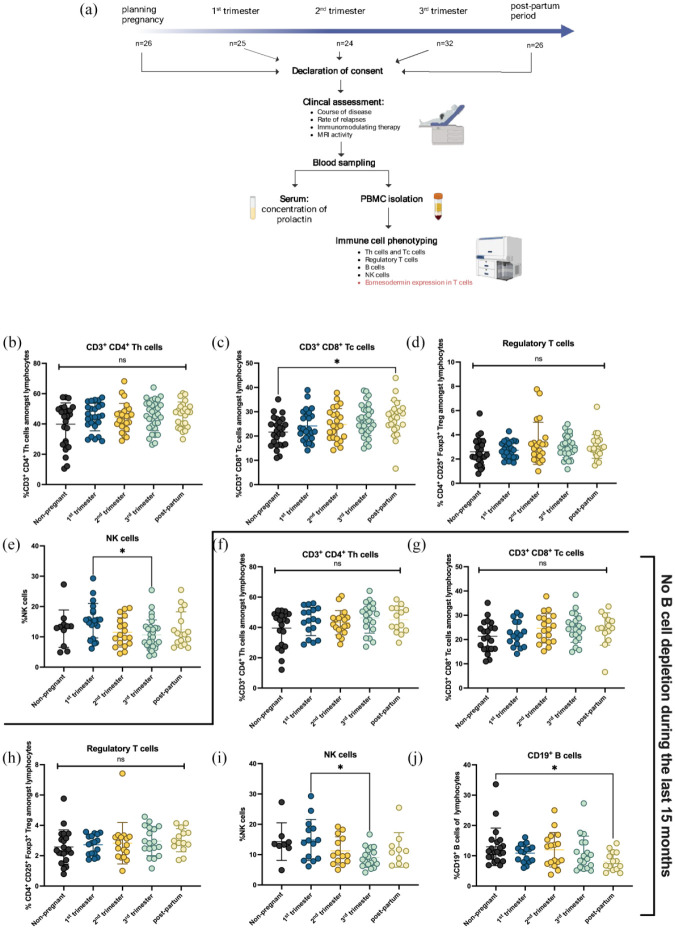
Methods: We enrolled n = 81 pregnant patients with relapsing-remitting MS (RRMS), n = 27 post-partum RRMS and n = 26 female RRMS control patients under the umbrella of the German Multiple Sclerosis and Pregnancy Registry. Clinical data were collected and immune cell alterations were analysed using flow cytometry.
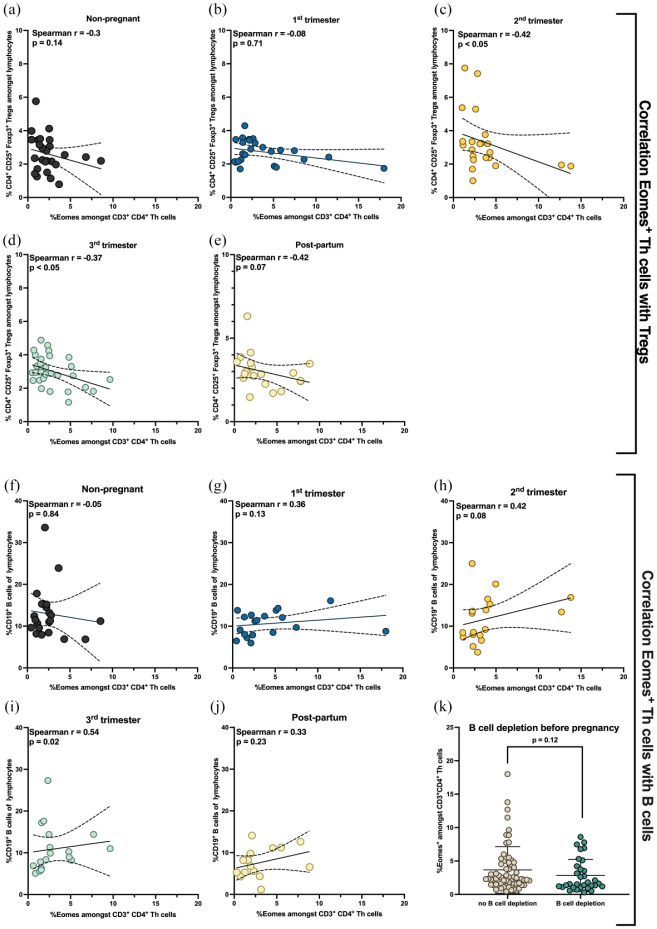
Results: While CD3+CD4+ Th cells were unaffected, CD3+CD8+ cytotoxic T-cells were elevated post-partum (p = 0.02) with reduced B-cell frequencies (p = 0.01) compared to non-pregnant RRMS patients. NK cells were elevated during first trimester (p = 0.02) compared to the third trimester. Frequencies of Eomes+ Th and Eomes+ Tc cells did not differ. There was no correlation of prolactin release and expression of Eomes+ Th cells. However, Eomes+ Th cells correlated with lower frequencies of regulatory T-cells during second (r = -0.42; p < 0.05) and third trimester (r = -0.37; p < 0.05). Moreover, Eomes+ Th cells correlated with frequencies of B-cells during third trimester (r = 0.54; p = 0.02). Frequencies of Eomes+ Th cells were not associated with the number of relapses before pregnancy, during pregnancy or post-partum. However, Eomes+ Th cells strongly correlated with disability post-partum as assessed using the EDSS (r = 0.52; p = 0.009).
Discussion: Pregnancy in MS is associated with robust immunological alterations. Eomes+ Th cells are capable of inducing immune cell alterations during the course of pregnancy, most evident during the second and third trimester as shown with a correlation of reduced Treg cells and a significant increase of B-cells. Importantly, Eomes+ Th cells correlate with disability post-partum. In summary, during late pregnancy in MS an inflammatory, cytotoxic and dysregulated immunological environment is primed gaining function post-delivery. This may be responsible for post-partum disability accumulation.
Keywords: Eomesodermin+ Th cells; multiple sclerosis; pregnancy; progression independent of relapse activity.
© The Author(s), 2024.
Conflict of interest statement
SF has received speaker’s and/or scientific board honoraria from AstraZeneca, Biogen, BMS, Celgene, Janssen, Merck, Novartis and Roche; and grant support from Ruhr-University Bochum, DMSG, Stiftung für therapeutische Forschung, Lead Discovery Center GmbH and Novartis. MB and PT have received funding from the FoRUM-program of the Medical Faculty of Ruhr-University Bochum. ST has nothing to disclose. TY has received speaker honoraria from Biogen, Novartis, Chugai, Takeda, Mitsubishi-Tanabe, Miyarisan and Sumitomo Pharma; serves on the editorial boards of Therapeutic Advances in Neurological Diseases and Clinical and Experimental Neuroimmunology; receives research support from Novartis and Chiome Bioscience; and receives royalties from EA Pharma. KH has received travel grants from Biogen, Novartis and Merck; and received speaker and research honoraria from Biogen Idec Germany, Teva, Sanofi Genzyme, Novartis, Bayer Health-Care, Merck Serono and Roche. RG serves on scientific advisory boards for Teva Pharmaceutical Industries Ltd., Biogen, Bayer Schering Pharma and Novartis; has received speaker honoraria from Biogen, Teva Pharmaceutical Industries Ltd., Bayer Schering Pharma and Novartis; serves as editor for Therapeutic Advances in Neurological Diseases and on the editorial boards of Experimental Neurology and the Journal of Neuroimmunology; and receives research support from Teva Pharmaceutical Industries Ltd., Biogen Idec, Bayer Schering Pharma, Genzyme, Merck Serono and Novartis. Because RG is Editor-in-Chief of this journal, the peer review process was managed by alternative members of the Board and the submitting Editor was not involved in the decision-making process.
Figures



Similar articles
-
Involvement of cytotoxic Eomes-expressing CD4+ T cells in secondary progressive multiple sclerosis.Proc Natl Acad Sci U S A. 2021 Mar 16;118(11):e2021818118. doi: 10.1073/pnas.2021818118. Proc Natl Acad Sci U S A. 2021. PMID: 33836594 Free PMC article.
-
Extrapituitary prolactin promotes generation of Eomes-positive helper T cells mediating neuroinflammation.Proc Natl Acad Sci U S A. 2019 Oct 15;116(42):21131-21139. doi: 10.1073/pnas.1906438116. Epub 2019 Sep 30. Proc Natl Acad Sci U S A. 2019. PMID: 31570595 Free PMC article.
-
Mitoxantrone: a review of its use in multiple sclerosis.CNS Drugs. 2004;18(6):379-96. doi: 10.2165/00023210-200418060-00010. CNS Drugs. 2004. PMID: 15089110 Review.
-
COPP-MS: COrticosteroids during the Post-Partum in relapsing Multiple Sclerosis patients.J Neurol. 2022 Oct;269(10):5571-5581. doi: 10.1007/s00415-022-11215-7. Epub 2022 Jun 23. J Neurol. 2022. PMID: 35737108
-
[Multiple sclerosis and pregnancy].Rev Neurol (Paris). 2006 Mar;162(3):299-309. doi: 10.1016/s0035-3787(06)75016-0. Rev Neurol (Paris). 2006. PMID: 16585885 Review. French.
References
-
- Orton SM, Herrera BM, Yee IM, et al.. Sex ratio of multiple sclerosis in Canada: a longitudinal study. Lancet Neurol 2006; 5: 932–936. - PubMed
-
- Confavreux C, Aimard G, Devic M. Course and prognosis of multiple sclerosis assessed by the computerized data processing of 349 patients. Brain 1980; 103: 281–300. - PubMed
-
- Confavreux C, Hutchinson M, Hours MM, et al.. Rate of pregnancy-related relapse in multiple sclerosis. Pregnancy in Multiple Sclerosis Group. N Engl J Med 1998; 339: 285–291. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
