

Higher Donor Age and Severe Microvascular Inflammation Are Risk Factors for Chronic Rejection After Treatment of Active Antibody-Mediated Rejection
- PMID: 38371907
- PMCID: PMC10869508
- DOI: 10.3389/ti.2024.11960
Higher Donor Age and Severe Microvascular Inflammation Are Risk Factors for Chronic Rejection After Treatment of Active Antibody-Mediated Rejection
Abstract
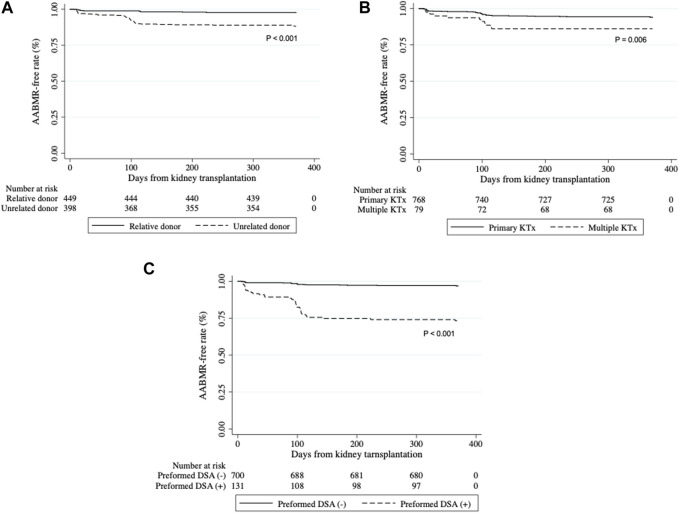
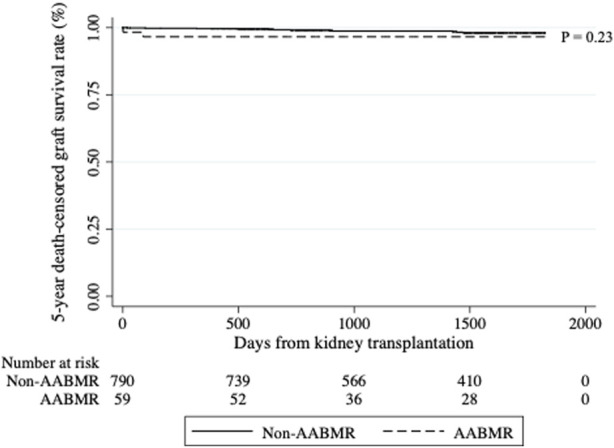
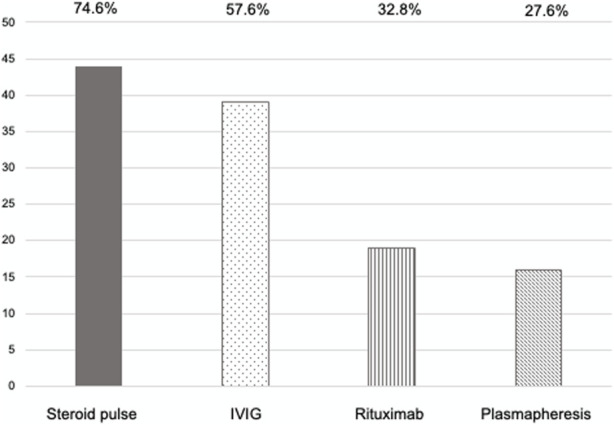
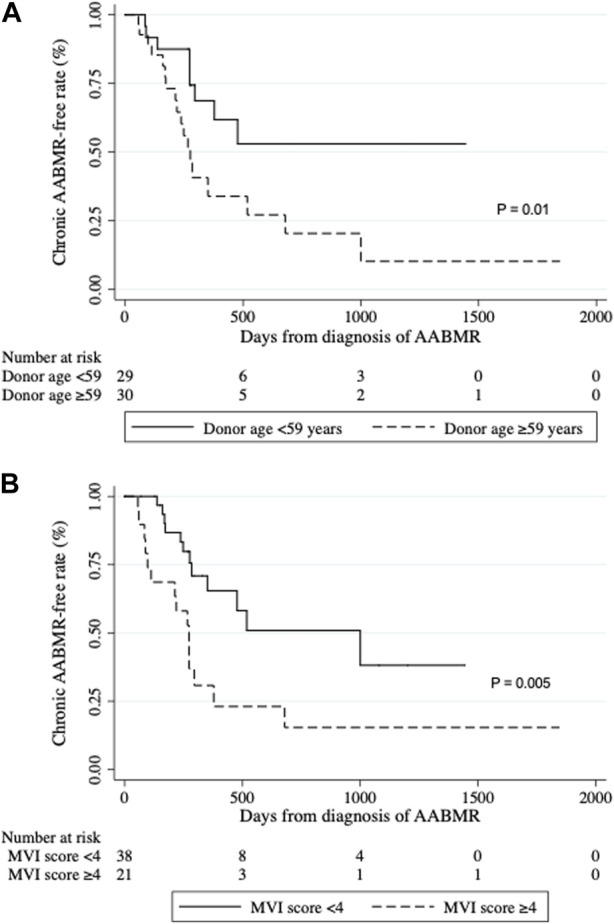
Recent developments in intensive desensitization protocols have enabled kidney transplantation in human leukocyte antigen (HLA)-sensitized recipients. However, cases of active antibody-mediated rejection (AABMR), when they occur, are difficult to manage, graft failure being the worst-case scenario. We aimed to assess the impact of our desensitization and AABMR treatment regimen and identify risk factors for disease progression. Among 849 patients who underwent living-donor kidney transplantation between 2014 and 2021 at our institution, 59 were diagnosed with AABMR within 1 year after transplantation. All patients received combination therapy consisting of steroid pulse therapy, intravenous immunoglobulin, rituximab, and plasmapheresis. Multivariable analysis revealed unrelated donors and preformed donor-specific antibodies as independent risk factors for AABMR. Five-year death-censored graft survival rate was not significantly different between patients with and without AABMR although 27 of 59 patients with AABMR developed chronic AABMR (CABMR) during the study period. Multivariate Cox proportional hazard regression analysis revealed that a donor age greater than 59 years and microvascular inflammation (MVI) score (g + ptc) ≥4 at AABMR diagnosis were independent risk factors for CABMR. Our combination therapy ameliorated AABMR; however, further treatment options should be considered to prevent CABMR, especially in patients with old donors and severe MVI.
Keywords: Banff classification; antibody-mediated rejection; graft survival; kidney transplantation; treatment outcomes.
Copyright © 2024 Banno, Hirai, Oki, Yagisawa, Unagami, Kanzawa, Omoto, Shimizu, Ishida and Takagi.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials