

Targeting Dendritic Cell Dysfunction to Circumvent Anti-PD1 Resistance in Head and Neck Cancer
- PMID: 38372707
- PMCID: PMC11061605
- DOI: 10.1158/1078-0432.CCR-23-3477
Targeting Dendritic Cell Dysfunction to Circumvent Anti-PD1 Resistance in Head and Neck Cancer
Abstract
Purpose: Neoadjuvant anti-PD1 (aPD1) therapies are being explored in surgically resectable head and neck squamous cell carcinoma (HNSCC). Encouraging responses have been observed, but further insights into the mechanisms underlying resistance and approaches to improve responses are needed.
Experimental design: We integrated data from syngeneic mouse oral carcinoma (MOC) models and neoadjuvant pembrolizumab HNSCC patient tumor RNA-sequencing data to explore the mechanism of aPD1 resistance. Tumors and tumor-draining lymph nodes (DLN) from MOC models were analyzed for antigen-specific priming. CCL5 expression was enforced in an aPD1-resistant model.
Results: An aPD1-resistant mouse model showed poor priming in the tumor DLN due to type 1 conventional dendritic cell (cDC1) dysfunction, which correlated with exhausted and poorly responsive antigen-specific T cells. Tumor microenvironment analysis also showed decreased cDC1 in aPD1-resistant tumors compared with sensitive tumors. Following neoadjuvant aPD1 therapy, pathologic responses in patients also positively correlated with baseline transcriptomic cDC1 signatures. In an aPD1-resistant model, intratumoral cDC1 vaccine was sufficient to restore aPD1 response by enhancing T-cell infiltration and increasing antigen-specific responses with improved tumor control. Mechanistically, CCL5 expression significantly correlated with neoadjuvant aPD1 response and enforced expression of CCL5 in an aPD1-resistant model, enhanced cDC1 tumor infiltration, restored antigen-specific responses, and recovered sensitivity to aPD1 treatment.
Conclusions: These data highlight the contribution of tumor-infiltrating cDC1 in HNSCC aPD1 response and approaches to enhance cDC1 infiltration and function that may circumvent aPD1 resistance in patients with HNSCC.
©2024 The Authors; Published by the American Association for Cancer Research.
Figures
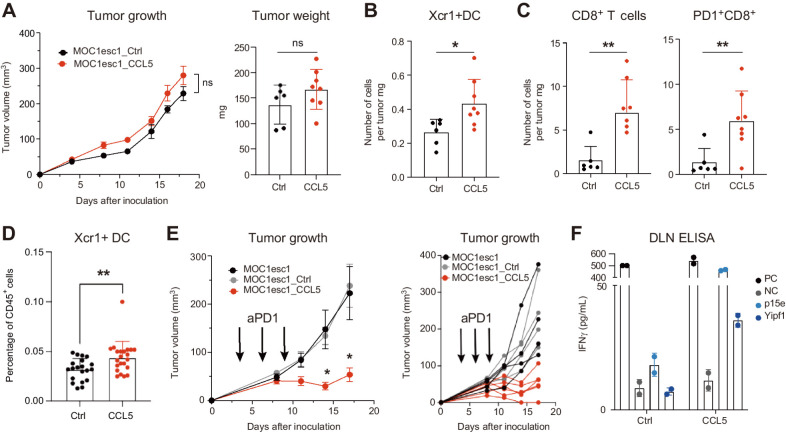
![Figure 4. CCL5 is highly expressed in aPD1-sensitive tumors. A, Heat map of CC chemokine ligands (CCL) based on pretreatment bulk RNA-seq data between responders (r) and nonresponders (nr). B, CCL5 mRNA expression comparison from bulk RNA-seq data of responders and nonresponders shown as z-score [n = 8 responders (r), n = 15 nonresponders (nr)]. C, CCL5 mRNA expression from bulk RNA-seq data of MOC22 tumors harvested on day 17, and MOC1P and MOC1-esc1 tumors harvested on day 14 after implantation shown as TPM (n = 3 each). D, Correlation of CCL5 mRNA expression (TPM) and cDC score (calculated from Xcell) in pretreatment bulk RNAseq data of HNSCC patient samples (n = 8 responders, n = 15 nonresponders). E, UMAP from scRNA-seq of pretreatment neoadjuvant pembrolizumab clinical trial patient tumors. (n = 2 each responder and nonresponder). F, Feature plots showing single-cell expression levels of CCL5 in responders and nonresponders. G, Distribution plots showing expression level of CCL5 in CD8+ T-cell subsets. Top, responders and bottom, nonresponders. H, Violin plots showing relative expression levels of CCL5 in responders versus nonresponders in baseline tumors. Individual data and mean are plotted in B, and individual data with mean ± SD are plotted in C. Data were analyzed using the Mann–Whitney U test to generate two-tailed P values in B, Pearson correlation coefficient in D. ***, P < 0.001.](https://cdn.ncbi.nlm.nih.gov/pmc/blobs/02a2/11061605/de1e545e404a/1934fig4.jpg)
Similar articles
-
Dendritic cell-based immunotherapy for head and neck squamous cell carcinoma: advances and challenges.Front Immunol. 2025 May 26;16:1573635. doi: 10.3389/fimmu.2025.1573635. eCollection 2025. Front Immunol. 2025. PMID: 40491907 Free PMC article. Review.
-
Enhanced oral versus flank lymph node T cell response parallels anti-PD1 efficacy in head and neck cancer.Oral Oncol. 2024 May;152:106795. doi: 10.1016/j.oraloncology.2024.106795. Epub 2024 Apr 9. Oral Oncol. 2024. PMID: 38599127 Free PMC article.
-
Tumor hypoxia is associated with resistance to PD-1 blockade in squamous cell carcinoma of the head and neck.J Immunother Cancer. 2021 May;9(5):e002088. doi: 10.1136/jitc-2020-002088. J Immunother Cancer. 2021. PMID: 33986123 Free PMC article.
-
Targeting resistance to radiation-immunotherapy in cold HNSCCs by modulating the Treg-dendritic cell axis.J Immunother Cancer. 2021 Apr;9(4):e001955. doi: 10.1136/jitc-2020-001955. J Immunother Cancer. 2021. PMID: 33883256 Free PMC article.
-
The Evolving Landscape of PD-1/PD-L1 Pathway in Head and Neck Cancer.Front Immunol. 2020 Sep 18;11:1721. doi: 10.3389/fimmu.2020.01721. eCollection 2020. Front Immunol. 2020. PMID: 33072064 Free PMC article. Review.
Cited by
-
Dendritic cell effector mechanisms and tumor immune microenvironment infiltration define TLR8 modulation and PD-1 blockade.Front Immunol. 2024 Dec 4;15:1440530. doi: 10.3389/fimmu.2024.1440530. eCollection 2024. Front Immunol. 2024. PMID: 39697344 Free PMC article. Clinical Trial.
-
The tumor-sentinel lymph node immuno-migratome reveals CCR7⁺ dendritic cells drive response to sequenced immunoradiotherapy.Nat Commun. 2025 Jul 17;16(1):6578. doi: 10.1038/s41467-025-61780-4. Nat Commun. 2025. PMID: 40675962 Free PMC article.
-
Dendritic cell-based immunotherapy for head and neck squamous cell carcinoma: advances and challenges.Front Immunol. 2025 May 26;16:1573635. doi: 10.3389/fimmu.2025.1573635. eCollection 2025. Front Immunol. 2025. PMID: 40491907 Free PMC article. Review.
-
Unraveling the immunomodulatory role of TIM-3 in head and neck squamous cell carcinoma: implications for targeted therapy.Discov Oncol. 2025 May 20;16(1):832. doi: 10.1007/s12672-025-02673-2. Discov Oncol. 2025. PMID: 40392355 Free PMC article. Review.
-
Dendritic cell effector mechanisms and tumor immune microenvironment infiltration define TLR8 modulation and PD-1 blockade.bioRxiv [Preprint]. 2024 Sep 6:2024.09.03.610636. doi: 10.1101/2024.09.03.610636. bioRxiv. 2024. Update in: Front Immunol. 2024 Dec 04;15:1440530. doi: 10.3389/fimmu.2024.1440530. PMID: 39282367 Free PMC article. Updated. Preprint.
References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. . Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021;71:209–49. - PubMed
-
- Cohen EEW, Soulières D, Le Tourneau C, Dinis J, Licitra L, Ahn MJ, et al. . Pembrolizumab versus methotrexate, docetaxel, or cetuximab for recurrent or metastatic head-and-neck squamous cell carcinoma (KEYNOTE-040): a randomised, open-label, phase 3 study. Lancet 2019;393:156–67. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
