

Long-term cardiovascular risks and the impact of statin treatment on socioeconomic inequalities: a microsimulation model
- PMID: 38373851
- PMCID: PMC10904120
- DOI: 10.3399/BJGP.2023.0198
Long-term cardiovascular risks and the impact of statin treatment on socioeconomic inequalities: a microsimulation model
Abstract
Background: UK cardiovascular disease (CVD) incidence and mortality have declined in recent decades but socioeconomic inequalities persist.
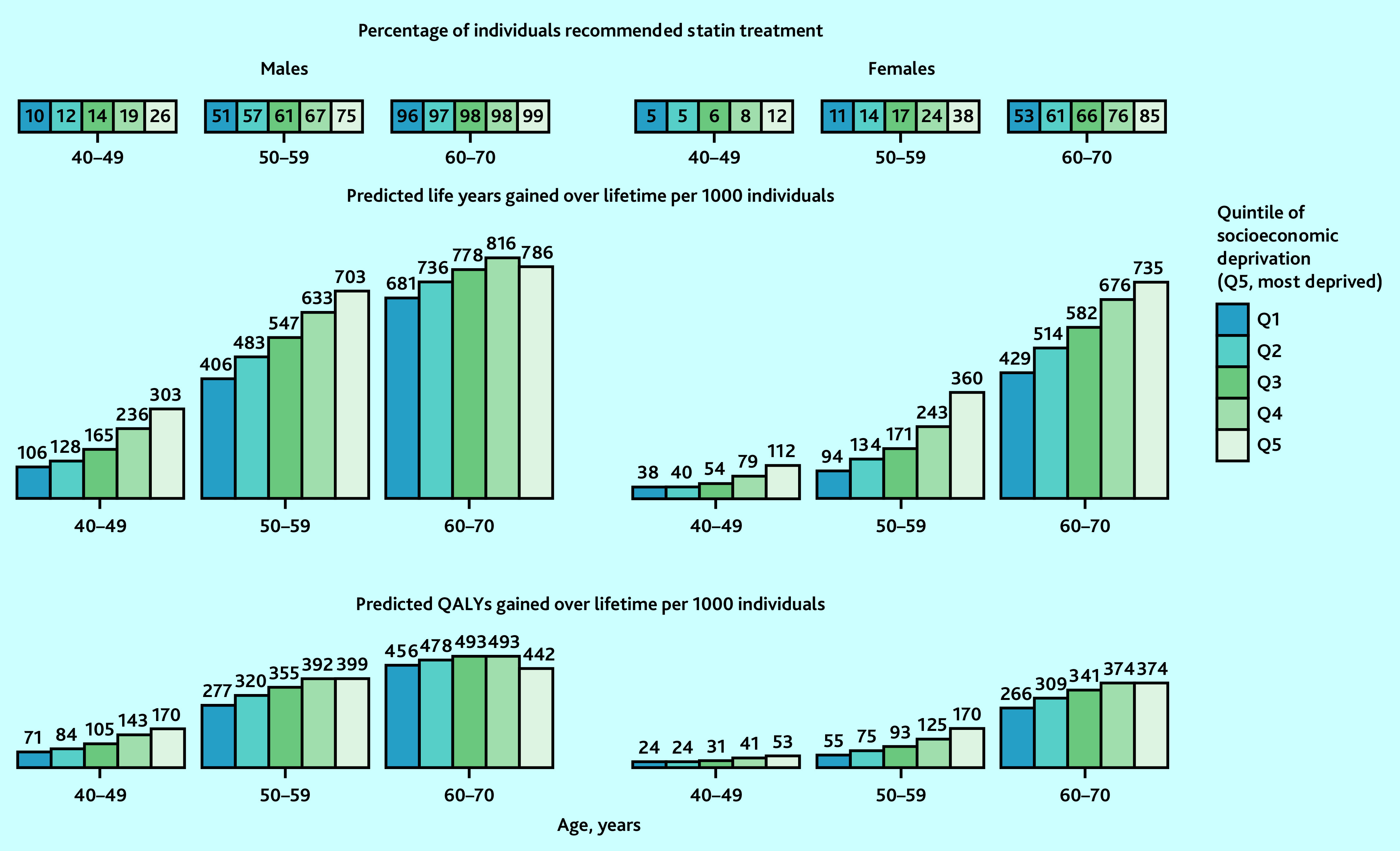
Aim: To present a new CVD model, and project health outcomes and the impact of guideline-recommended statin treatment across quintiles of socioeconomic deprivation in the UK.
Design and setting: A lifetime microsimulation model was developed using 117 896 participants in 16 statin trials, 501 854 UK Biobank (UKB) participants, and quality-of-life data from national health surveys.
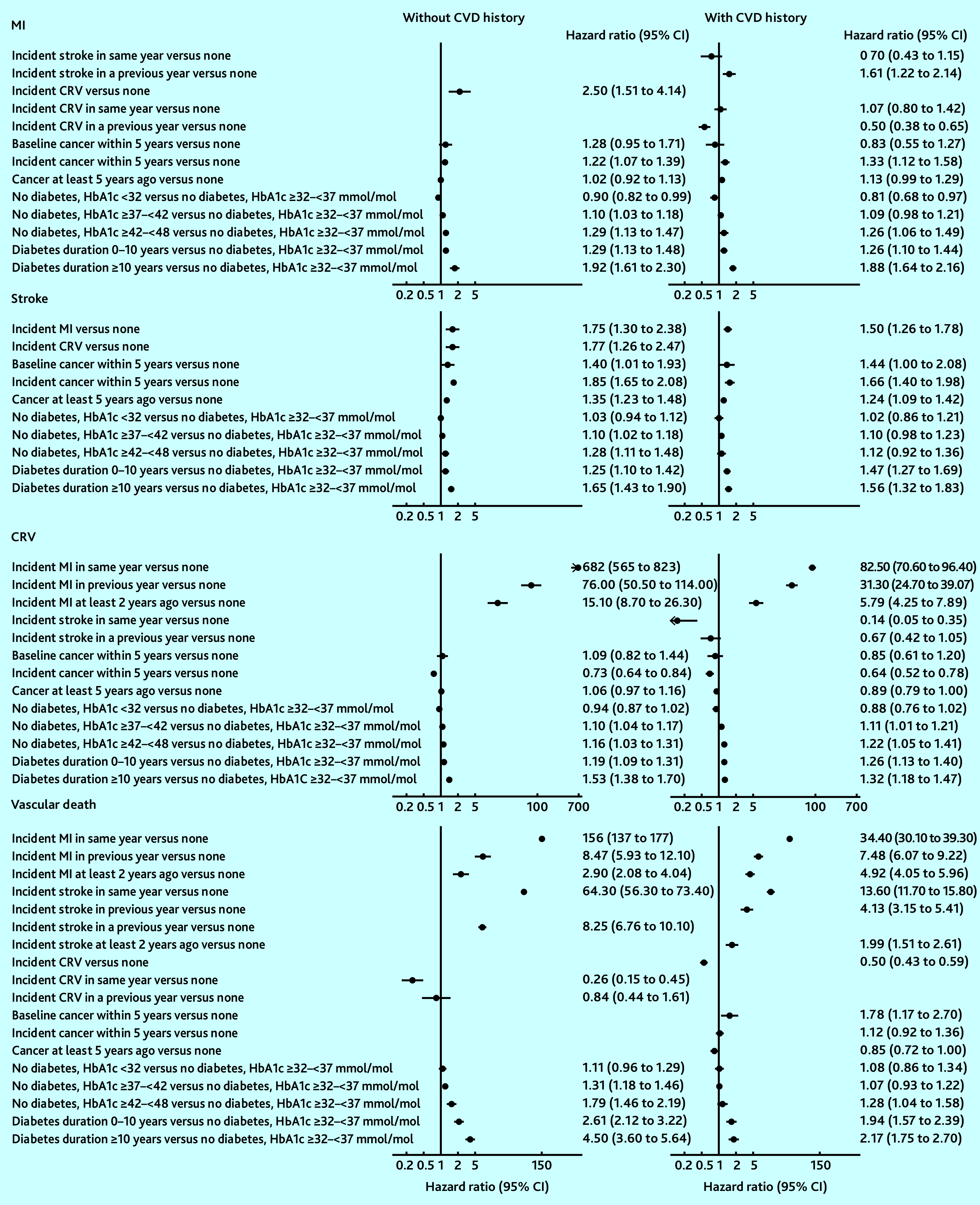
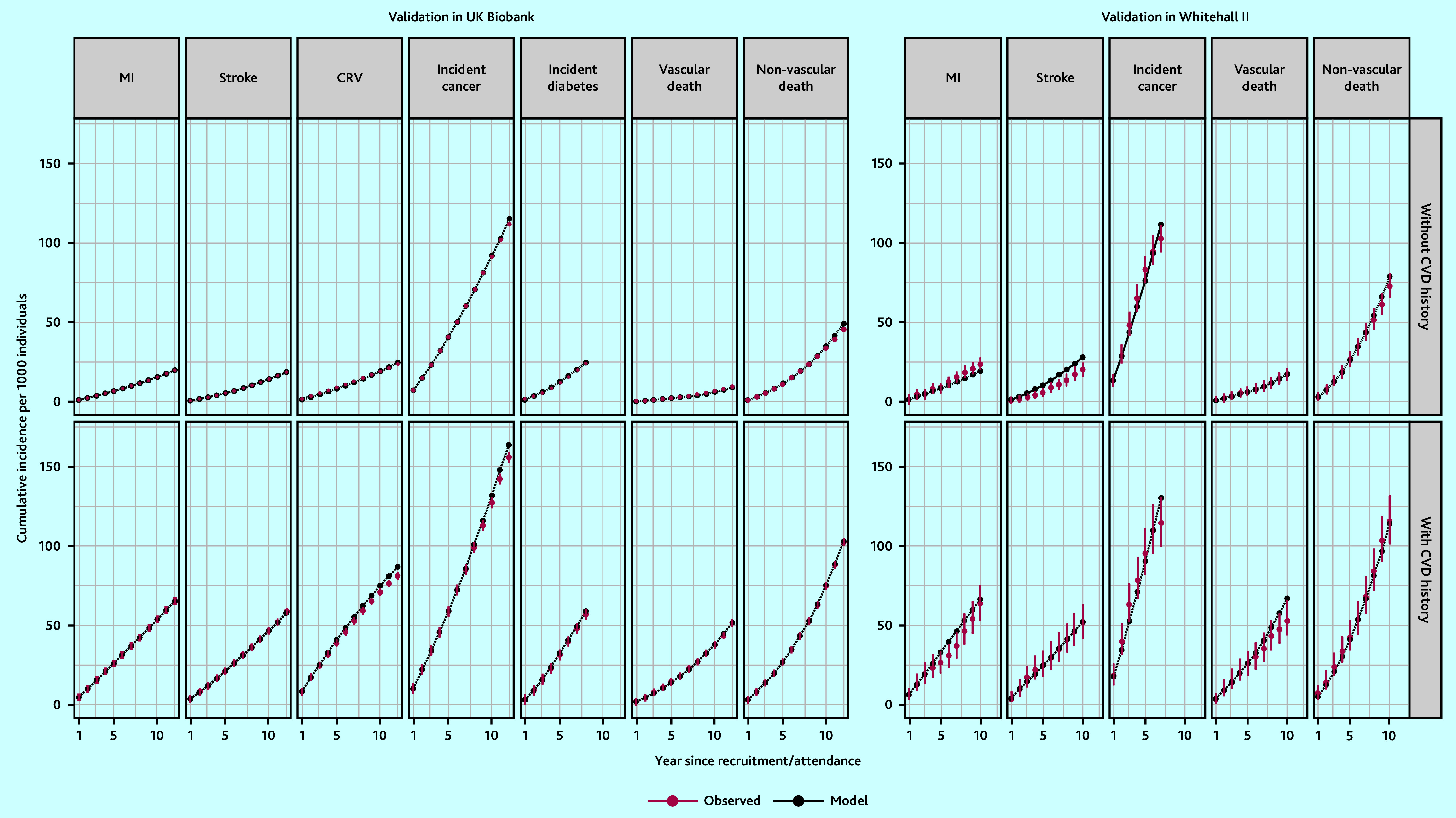
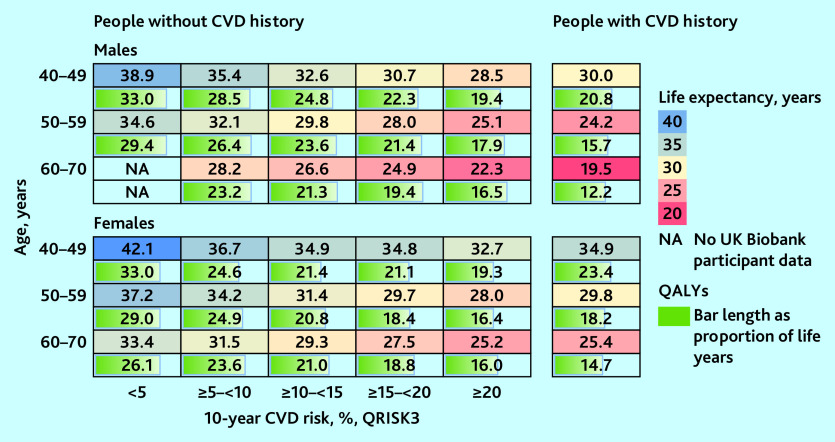
Method: A CVD microsimulation model was developed using risk equations for myocardial infarction, stroke, coronary revascularisation, cancer, and vascular and non-vascular death, estimated using trial data. The authors calibrated and further developed this model in the UKB cohort, including further characteristics and a diabetes risk equation, and validated the model in UKB and Whitehall II cohorts. The model was used to predict CVD incidence, life expectancy, quality-adjusted life years (QALYs), and the impact of UK guideline-recommended statin treatment across socioeconomic deprivation quintiles.
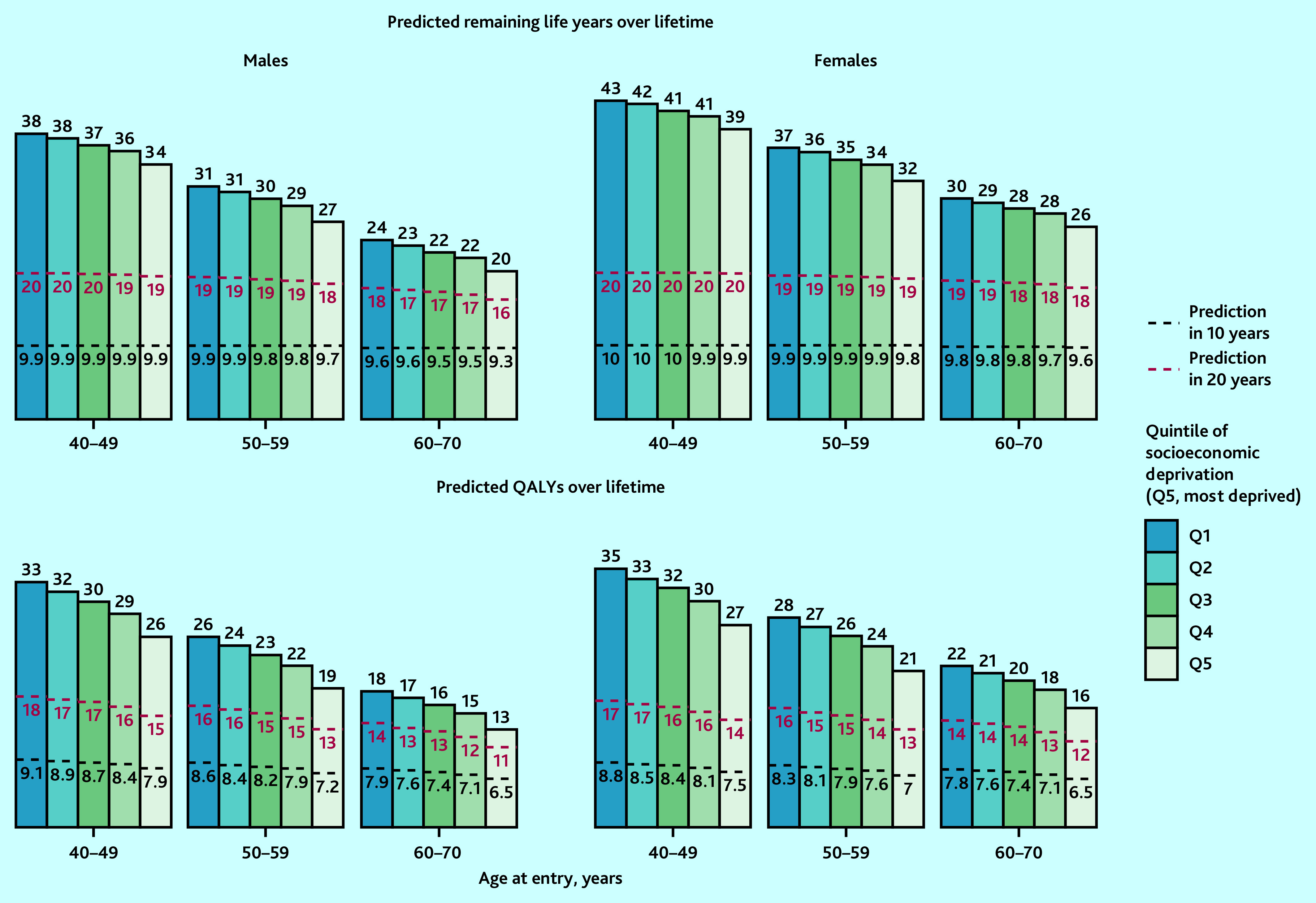
Results: Age, sex, socioeconomic deprivation, smoking, hypertension, diabetes, and cardiovascular events were key CVD risk determinants. Model-predicted event rates corresponded well to observed rates across participant categories. The model projected strong gradients in remaining life expectancy, with 4-5-year (5-8 QALYs) gaps between the least and most socioeconomically deprived quintiles. Guideline-recommended statin treatment was projected to increase QALYs, with larger gains in quintiles of higher deprivation.
Conclusion: The study demonstrated the potential of guideline-recommended statin treatment to reduce socioeconomic inequalities. This CVD model is a novel resource for individualised long-term projections of health outcomes of CVD treatments.
Keywords: Markov microsimulation model; cardiovascular disease; individual patient characteristics; inequality; quality-adjusted life years; socioeconomic status.
© The Authors.
Conflict of interest statement
Anthony Keech reports research support from Abbott, Amgen, ASPEN, Bayer, Mylan, Novartis, Sanofi, and Viatris; speaker fees from Novartis; and is a Data Safety Monitoring Board member for Kowa. John Robson reports funding from North East London Integrated Care Service. Jane Armitage reports receiving a grant to their research institution from Novartis for the ORION 4 trial of inclisiran. John Simes reports receiving grants for his institution from Amgen, Bayer, BMS, MSD, Pfizer, and Roche; consulting fees from FivepHusion; and is a chair (unpaid) of STAREE DSMB. Colin Baigent reports research grants from Boehringer Ingelheim and Health Data Research UK, and is a chair (unpaid) of a Data Safety Monitoring Board for Merck. All other authors have declared no competing interests.
Figures
References
-
- World Health Organization Cardiovascular diseases (CVDs) 2021. https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases... (accessed 29 Jan 2024).
-
- Marmot M, Allen J, Boyce T, et al. Health equity in England: the Marmot review 10 years on. 2020 https://www.health.org.uk/publications/reports/the-marmot-review-10-year... (accessed 29 Jan 2024). - PubMed
-
- Briggs A, Sculpher M, Claxton K. Decision modelling for health economic evaluation. Oxford: Oxford University Press; 2006.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical