

Inflammatory markers and frailty in home-dwelling elderly, a cross-sectional study
- PMID: 38373890
- PMCID: PMC10877806
- DOI: 10.1186/s12877-024-04690-2
Inflammatory markers and frailty in home-dwelling elderly, a cross-sectional study
Abstract
Background: Low-grade, chronic inflammation during ageing, ("inflammageing"), is suggested to be involved in the development of frailty in older age. However, studies on the association between frailty, using the frailty index definition, and inflammatory markers are limited. The aim of this study was to investigate the relationship between inflammatory markers and frailty index (FI) in older, home-dwelling adults.
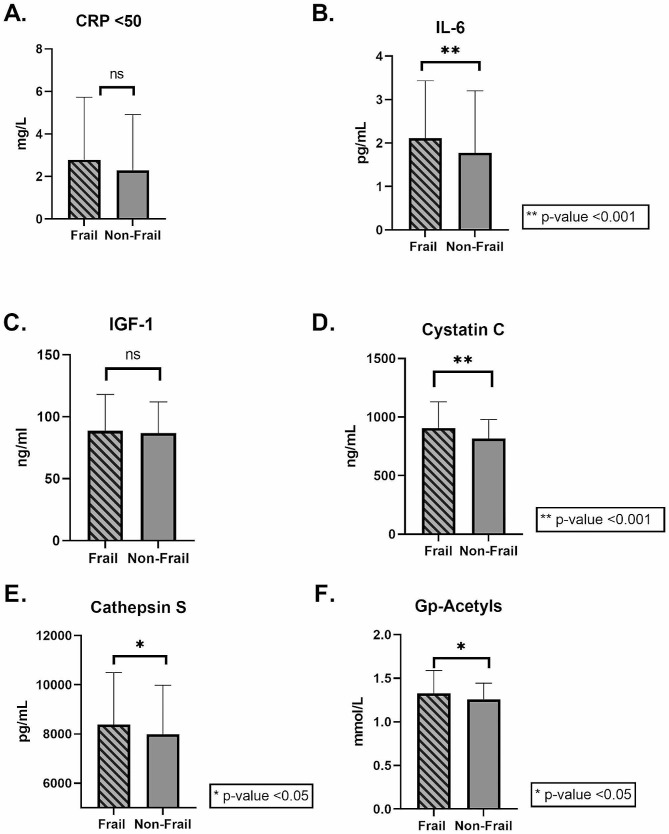
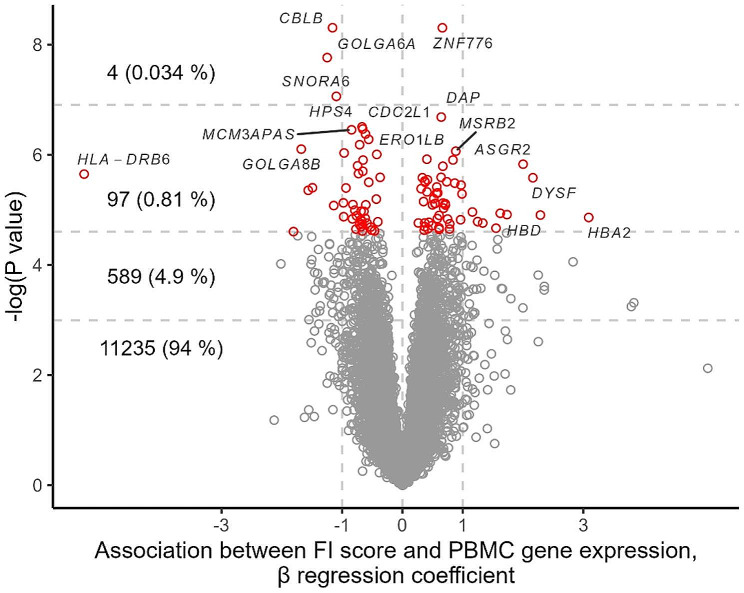
Method: Home-dwelling men and women aged ≥ 70 years old, living in South-East Norway were recruited and included in a cross-sectional study. The FI used in the current study was developed according to Rockwood's frailty index and included 38 variables, resulting in an FI score between 0 and 1 for each participant. Circulating inflammatory markers (IL-6, CRP, IGF-1, cystatin C, cathepsin S, and glycoprotein Acetyls) were analyzed from non-fasting blood samples using ELISA. Whole-genome PBMC transcriptomics was used to study the association between FI score and inflammation.
Results: The study population comprised 403 elderly (52% women), with a median age of 74 years and a mean BMI of 26.2 kg/m2. The mean FI score for the total group was 0.15 (range 0.005-0.56). The group was divided into a frail group (FI score ≥ 0.25) and non-frail group. After adjusting for BMI, age, sex, and smoking in the whole group, IL-6, cathepsin S, cystatin C, and Gp-acetyls remained significant associated to FI score (IL-6: 0.002, 95% CI: 0.001, 0.002, cathepsin S: 6.7e-06, 95% CI 2.44e-06, 0.00001, cystatin C: 0.004, 95% CI: 0.002, 0.006, Gp- Acetyls: 0.09, 95% CI: 0.05, 0.13, p < 0.01 for all), while CRP and IGF-1 were not (0.0003, 95% CI: -00001, 0.0007, p = 0.13, (-1.27e-06), 95% CI: (-0.0003), 0.0003, p = 0.99). There was a significant association between FI score and inflammatory markers, and FI score and monocyte-specific gene expression.
Conclusions: We found an association between FI score and inflammatory markers, and between FI score and monocyte-specific gene expression among elderly subjects above 70 years of age. Whether inflammation is a cause or consequence of frailty and whether the progression of frailty can be attenuated by reducing inflammation remains to be clarified.
Keywords: Ageing; Cross-sectional; Frailty; Frailty Index; Gene expression; Home-dwelling; Inflammageing; Inflammation; PBMC.
© 2024. The Author(s).
Conflict of interest statement
During the past 5 years, S. M. U. has received research grants from Mills DA and Olympic Seafood, none of which are related to the content of this manuscript. During the past 5 years, K. B. H. has received research grants or honoraria from Sanofi, not related to the contents of this manuscript. J.J.C. has received research grants and/or personal fees from Mills DA, none of which is related to the content of this manuscript. P.B. and I.O. has no conflict of interest.
Figures



References
-
- WHO. Ageing and health www.who.int: World Health Organization (WHO); 2022 [updated 1. October 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
Miscellaneous
