

A prospective study to evaluate the contribution of the pediatric appendicitis score in the decision process
- PMID: 38373918
- PMCID: PMC10875762
- DOI: 10.1186/s12887-024-04619-z
A prospective study to evaluate the contribution of the pediatric appendicitis score in the decision process
Abstract
Background: The objective of this study was to assess the likelihood of acute appendicitis (AA) in children presenting with abdominal symptoms at the emergency department (ED), based on their prior primary care (PC) consultation history.
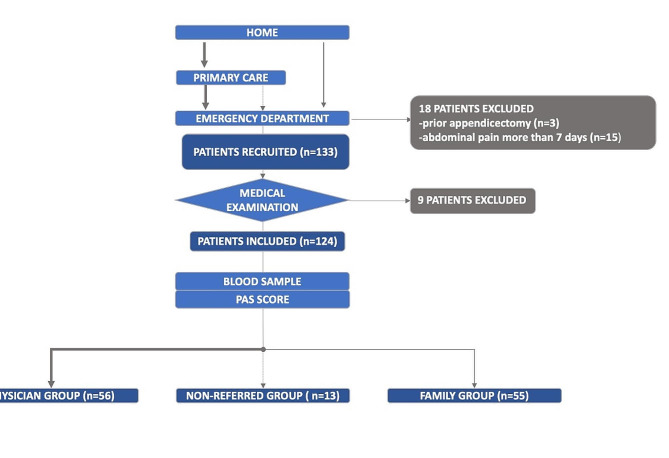
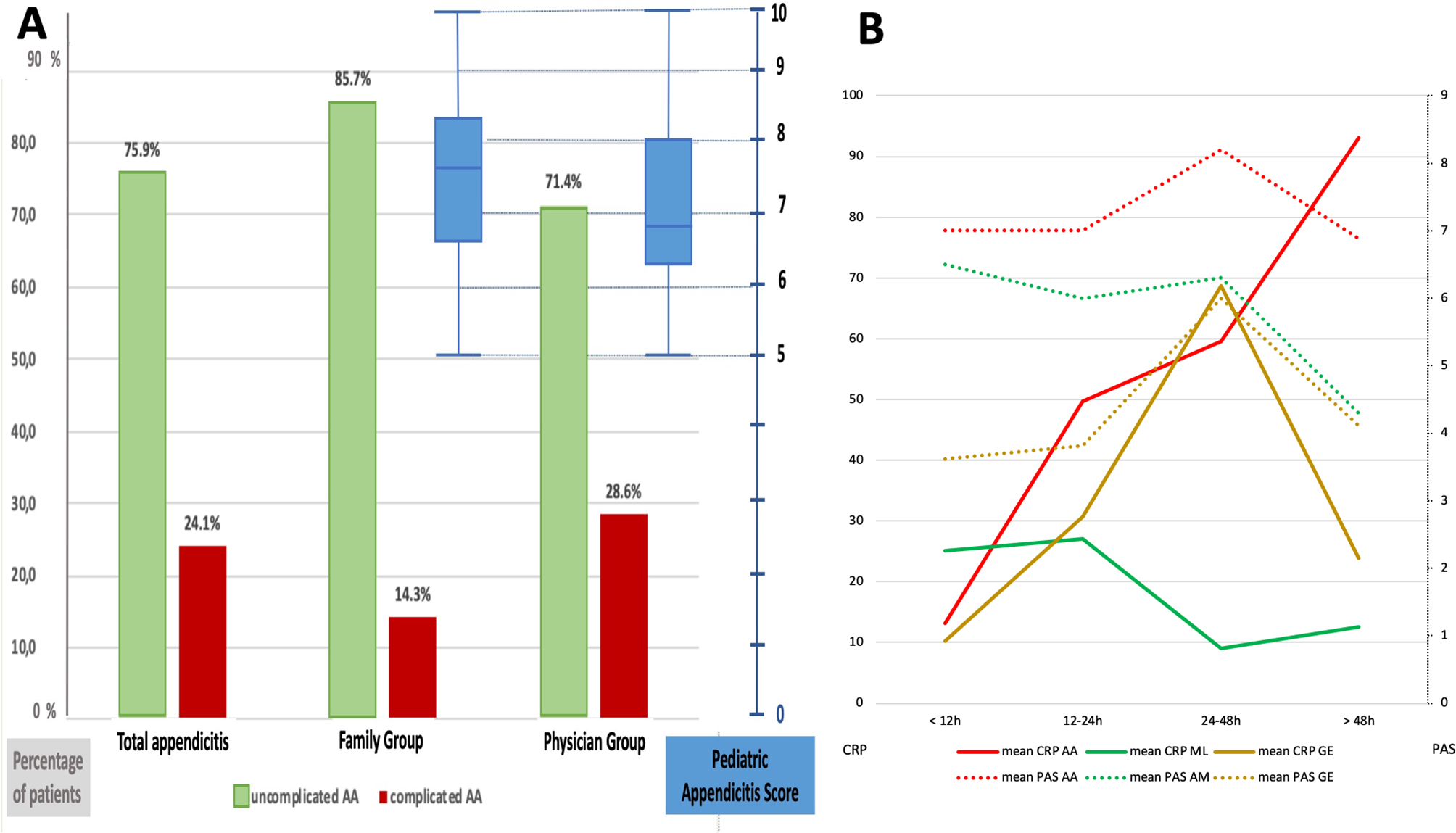
Methods: Between February and June 2021, we prospectively enrolled all children presenting at the ED with acute abdominal pain indicative of possible acute appendicitis (AA). Subsequently, they were categorized into three groups: those assessed by a PC physician (PG), those brought in by their family without a prior consultation (FG), and those admitted after a PC consultation without being assessed as such. The primary objective was to assess the probability of AA diagnosis using the Pediatric Appendicitis Score (PAS). Secondary objectives included analyzing PAS and C-reactive protein (CRP) levels based on the duration of pain and final diagnoses.
Results: 124 children were enrolled in the study (PG, n = 56; FG, n = 55; NG, n = 13). Among them, 29 patients (23.4%) were diagnosed with AA, with 13 cases (23.2%) from the PG and 14 cases (25.4%) from the FG. The mean PAS scores for AA cases from the PG and FG were 6.69 ± 1.75 and 7.57 ± 1.6, respectively, (p = 0.3340). Both PAS scores and CRP levels showed a significant correlation with AA severity. No cases of AA were observed with PAS scores < 4.
Conclusions: There was no significant difference in PAS scores between patients addressed by PG and FG, even though PAS scores tended to be higher for patients with AA. We propose a new decision-making algorithm for PC practice, which incorporates inflammatory markers and pain duration.
Trial registration: Institutional Ethics Committee registration number: 447-2021-103 (10/01/2021).
Clinical trials registration number: ClinicalTrials.gov Identifier: NCT04885335 (Registered on 13/05/2021).
Keywords: Acute appendicitis; Children; Emergency; PAS score; Primary care.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Vons C, Brami M. Épidémiologie descriptive des appendicites en France: Faut-Il revoir la physiopathologie des appendicites aiguës? Bull Académie Natl Médecine. 2017;201:339–57. doi: 10.1016/S0001-4079(19)30505-9. - DOI
-
- Andersen SB, Paerregaard A, Larsen K. Changes in the epidemiology of acute appendicitis and appendectomy in Danish children 1996–2004. Eur J Pediatr Surg off J Austrian Assoc Pediatr Surg Al Z Kinderchir. 2009;19:286–9. - PubMed
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
