

Post-transplant cyclophosphamide versus anti-thymocyte globulin after reduced intensity peripheral blood allogeneic cell transplantation in recipients of matched sibling or 10/10 HLA matched unrelated donors: final analysis of a randomized, open-label, multicenter, phase 2 trial
- PMID: 38374026
- PMCID: PMC10876658
- DOI: 10.1038/s41408-024-00990-3
Post-transplant cyclophosphamide versus anti-thymocyte globulin after reduced intensity peripheral blood allogeneic cell transplantation in recipients of matched sibling or 10/10 HLA matched unrelated donors: final analysis of a randomized, open-label, multicenter, phase 2 trial
Abstract
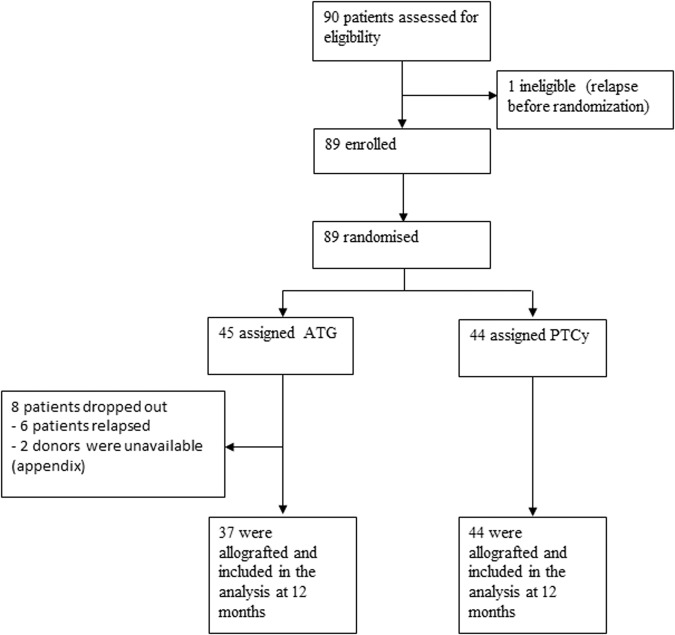
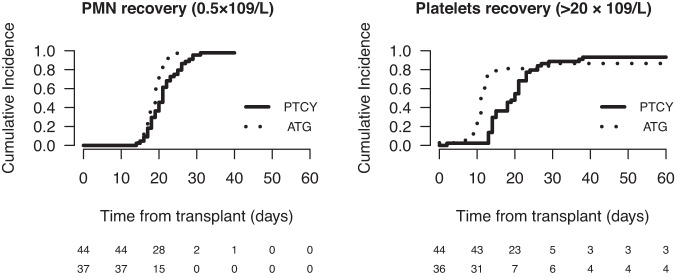
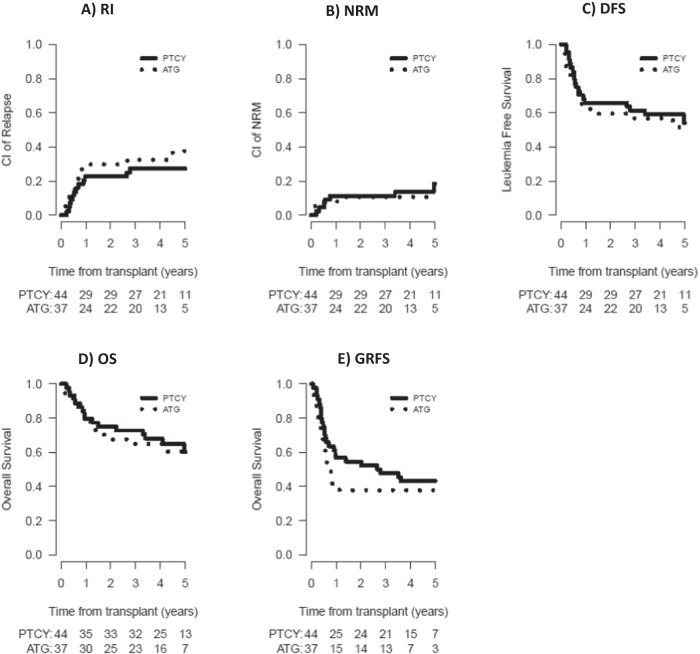
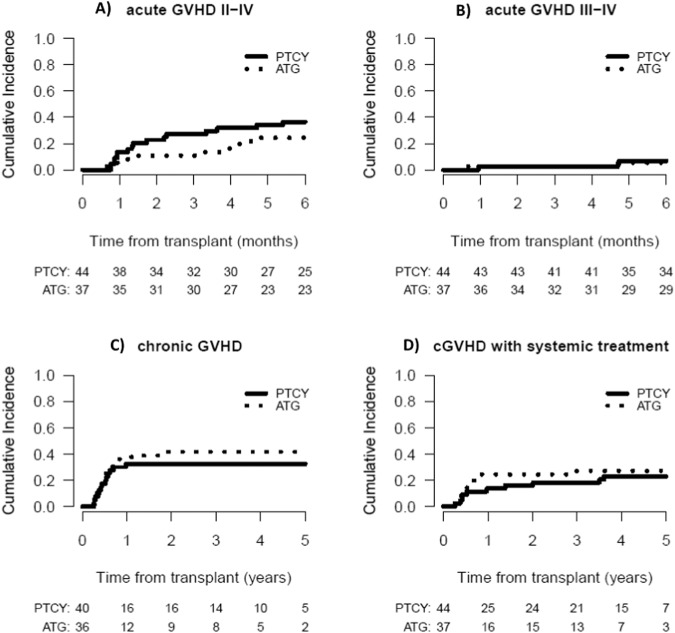
The use of post-transplantation cyclophosphamide (PTCy) for graft-versus-host disease (GVHD) prophylaxis is not established after reduced intensity conditioning (RIC) hematopoietic stem cell transplantation (HSCT) from fully matched donors. This was a randomized, open-label, multicenter, phase 2 trial. All patients received a RIC regimen with fludarabine, intravenous busulfan for 2 days (Flu-Bu2), and a peripheral blood stem cell (PBSC) graft from a matched related or 10/10 HLA-matched unrelated donor. Patients were randomly assigned to receive anti-thymocyte globulin (ATG) 5 mg/kg plus standard GVHD prophylaxis or PTCy 50 mg/kg/d at days +3 and +4 plus standard GVHD prophylaxis. The primary endpoint was the composite endpoint of GVHD- and relapse-free survival (GRFS) at 12 months after HSCT. Eighty-nine patients were randomly assigned to receive either PTCy or control prophylaxis with ATG. At 12 months, disease-free survival was 65.9% in the PTCy group and 67.6% in the ATG group (P = 0.99). Cumulative incidence of relapse, non-relapse mortality, and overall survival were also comparable in the two groups. GRFS at 12 months was 54.5% in the PTCy group versus 43.2% in the ATG group (P = 0.27). The median time to neutrophil and platelet count recovery was significantly longer in the PTCy group compared to the ATG group. Except for day +30, where EORTC QLQ-C30 scores were significantly lower in the PTCy compared to the ATG group, the evolution with time was not different between the two groups. Although the primary objective was not met, PTCy is effective for GVHD prophylaxis in patients receiving Flu-Bu2 conditioning with a PBSC graft from a fully matched donor and was well tolerated in term of adverse events and quality of life. This trial was registered at clinicaltrials.gov: NCT02876679.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Passweg JR, Baldomero H, Chabannon C, Basak GW, de la Camara R, Corbacioglu S, et al. Hematopoietic cell transplantation and cellular therapy survey of the EBMT: monitoring of activities and trends over 30 years. Bone Marrow Transpl. 2021;56:1651–64. doi: 10.1038/s41409-021-01227-8. - DOI - PMC - PubMed
-
- Mohty M, Bay JO, Faucher C, Choufi B, Bilger K, Tournilhac O, et al. Graft-versus-host disease following allogeneic transplantation from HLA-identical sibling with antithymocyte globulin-based reduced-intensity preparative regimen. Blood. 2003;102:470–6. doi: 10.1182/blood-2002-12-3629. - DOI - PubMed
-
- Yafour N, Serradj F, Osmani S, Brahimi M, Bouhass R, Arabi A, et al. Improving survival rates for patients with acute myeloid leukemia: Impacts of fludarabine/busulfan and antithymocyte globulin as reduced toxicity myeloablative conditioning for matched related donor allo-HCT. Curr Res Transl Med. 2020;68:145–8. - PubMed
-
- Le Bourgeois A, Lestang E, Guillaume T, Delaunay J, Ayari S, Blin N, et al. Prognostic impact of immune status and hematopoietic recovery before and after fludarabine, IV busulfan, and antithymocyte globulins (FB2 regimen) reduced-intensity conditioning regimen (RIC) allogeneic stem cell transplantation (allo-SCT) Eur J Haematol. 2013;90:177–86. doi: 10.1111/ejh.12049. - DOI - PubMed
-
- Blaise D, Tabrizi R, Boher JM, Le Corroller-Soriano AG, Bay JO, Fegueux N, et al. Randomized study of 2 reduced-intensity conditioning strategies for human leukocyte antigen-matched, related allogeneic peripheral blood stem cell transplantation: prospective clinical and socioeconomic evaluation. Cancer. 2013;119:602–11. doi: 10.1002/cncr.27786. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
