

Clonal chromosomal mosaicism and loss of chromosome Y in elderly men increase vulnerability for SARS-CoV-2
- PMID: 38374351
- PMCID: PMC10876565
- DOI: 10.1038/s42003-024-05805-6
Clonal chromosomal mosaicism and loss of chromosome Y in elderly men increase vulnerability for SARS-CoV-2
Abstract
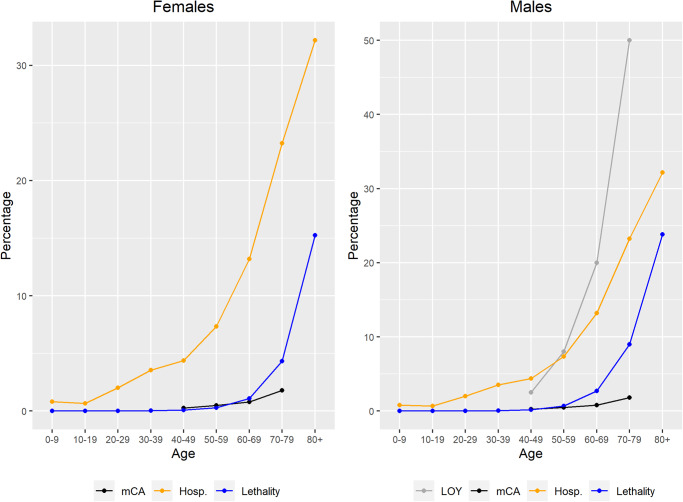
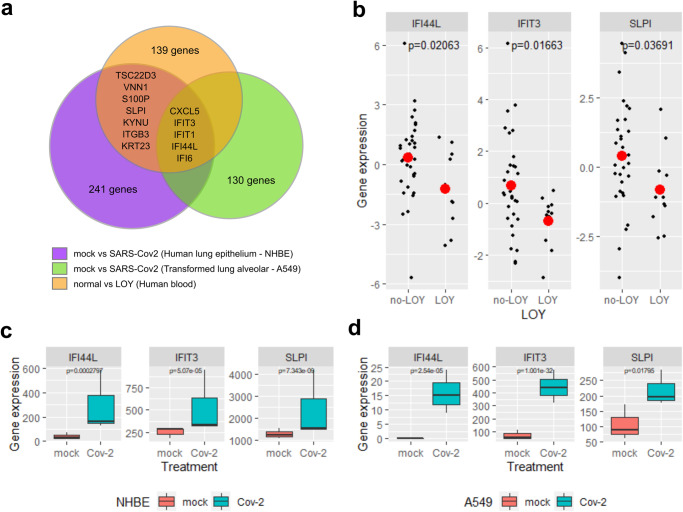
The pandemic caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2, COVID-19) had an estimated overall case fatality ratio of 1.38% (pre-vaccination), being 53% higher in males and increasing exponentially with age. Among 9578 individuals diagnosed with COVID-19 in the SCOURGE study, we found 133 cases (1.42%) with detectable clonal mosaicism for chromosome alterations (mCA) and 226 males (5.08%) with acquired loss of chromosome Y (LOY). Individuals with clonal mosaic events (mCA and/or LOY) showed a 54% increase in the risk of COVID-19 lethality. LOY is associated with transcriptomic biomarkers of immune dysfunction, pro-coagulation activity and cardiovascular risk. Interferon-induced genes involved in the initial immune response to SARS-CoV-2 are also down-regulated in LOY. Thus, mCA and LOY underlie at least part of the sex-biased severity and mortality of COVID-19 in aging patients. Given its potential therapeutic and prognostic relevance, evaluation of clonal mosaicism should be implemented as biomarker of COVID-19 severity in elderly people.
© 2024. The Author(s).
Conflict of interest statement
LAPJ is founding partner and scientific advisor of qGenomics laboratories. The other authors declare no competing interests.
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
