

Missingness matters: a secondary analysis of thromboelastography measurements from a recent prehospital randomized tranexamic acid clinical trial
- PMID: 38375027
- PMCID: PMC10875568
- DOI: 10.1136/tsaco-2023-001346
Missingness matters: a secondary analysis of thromboelastography measurements from a recent prehospital randomized tranexamic acid clinical trial
Abstract
Background: Tranexamic acid (TXA) has been hypothesized to mitigate coagulopathy in patients after traumatic injury. Despite previous prehospital clinical trials demonstrating a TXA survival benefit, none have demonstrated correlated changes in thromboelastography (TEG) parameters. We sought to analyze if missing TEG data contributed to this paucity of findings.
Methods: We performed a secondary analysis of the Study of Tranexamic Acid During Air Medical and Ground Prehospital Transport Trial. We compared patients that received TEG (YES-TEG) and patients unable to be sampled (NO-TEG) to analyze subgroups in which to investigate TEG differences. TEG parameter differences across TXA intervention arms were assessed within subgroups disproportionately present in the NO-TEG relative to the YES-TEG cohort. Generalized linear models controlling for potential confounders were applied to findings with p<0.10 on univariate analysis.
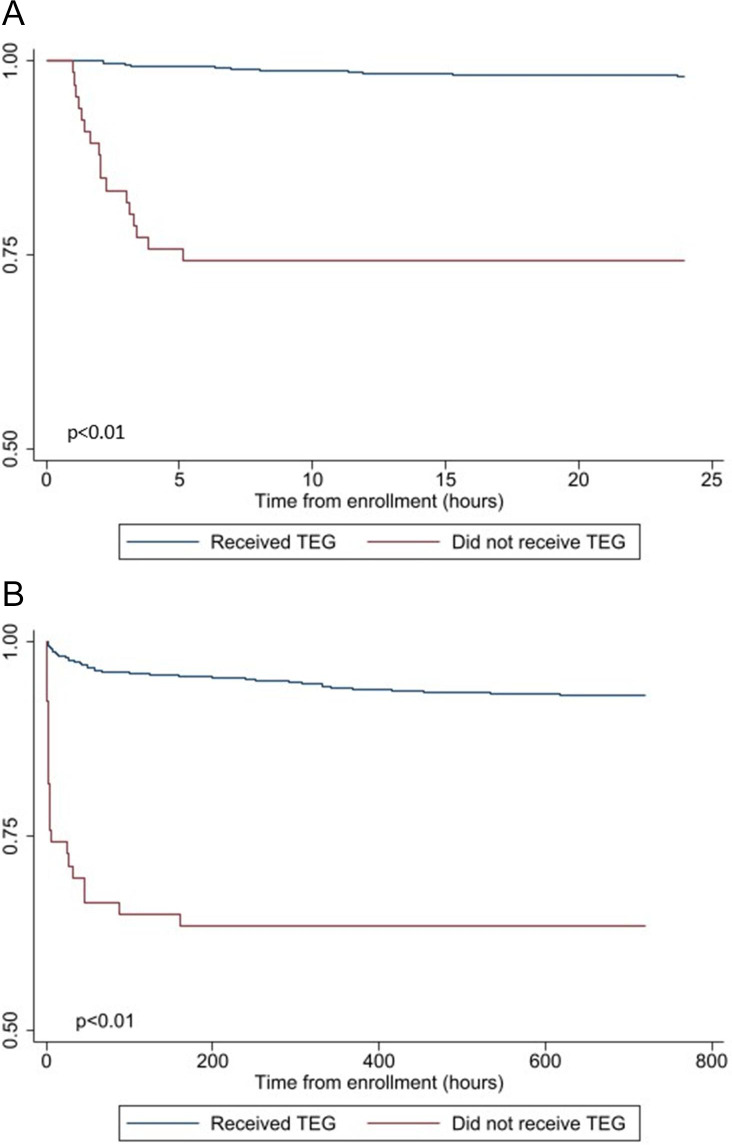
Results: NO-TEG patients had lower prehospital systolic blood pressure (SBP) (100 (78, 140) vs 125 (88, 147), p<0.01), lower prehospital Glascow Coma Score (14 (3, 15) vs 15 (12, 15), p<0.01), greater rates of prehospital intubation (39.4% vs 24.4%, p<0.01) and greater mortality at 30 days (36.4% vs 6.8%, p<0.01). NO-TEG patients had a greater international normalized ratio relative to the YES-TEG subgroup (1.2 (1.1, 1.5) vs 1.1 (1.0, 1.2), p=0.04). Within a severe prehospital shock cohort (SBP<70), TXA was associated with a significant decrease in clot lysis at 30 min on multivariate analysis (β=-27.6, 95% CI (-51.3 to -3.9), p=0.02).
Conclusions: Missing data, due to the logistical challenges of sampling certain severely injured patients, may be associated with a lack of TEG parameter changes on TXA administration in the primary analysis. Previous demonstration of TXA's survival benefit in patients with severe prehospital shock in tandem with the current findings supports the notion that TXA acts at least partially by improving clot integrity.
Level of evidence: Level II.
Keywords: Multiple Trauma; blood transfusion; thromboelastography; tranexamic acid.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Lost and found: how missing data connects TXA and outcomes in severely injured patients.Trauma Surg Acute Care Open. 2024 Mar 7;9(1):e001429. doi: 10.1136/tsaco-2024-001429. eCollection 2024. Trauma Surg Acute Care Open. 2024. PMID: 38464550 Free PMC article. No abstract available.
-
What you don't know can hurt you: a statistical commentary on missing data in trauma research.Trauma Surg Acute Care Open. 2024 Apr 2;9(1):e001405. doi: 10.1136/tsaco-2024-001405. eCollection 2024. Trauma Surg Acute Care Open. 2024. PMID: 38571726 Free PMC article. No abstract available.
Similar articles
-
Tranexamic acid administration in the field does not affect admission thromboelastography after traumatic brain injury.J Trauma Acute Care Surg. 2020 Nov;89(5):900-907. doi: 10.1097/TA.0000000000002932. J Trauma Acute Care Surg. 2020. PMID: 33105308 Free PMC article. Clinical Trial.
-
Prehospital synergy: Tranexamic acid and blood transfusion in patients at risk for hemorrhage.J Trauma Acute Care Surg. 2022 Jul 1;93(1):52-58. doi: 10.1097/TA.0000000000003620. Epub 2022 Apr 8. J Trauma Acute Care Surg. 2022. PMID: 35393385 Free PMC article. Clinical Trial.
-
Early Prehospital Tranexamic Acid Following Injury Is Associated With a 30-day Survival Benefit: A Secondary Analysis of a Randomized Clinical Trial.Ann Surg. 2021 Sep 1;274(3):419-426. doi: 10.1097/SLA.0000000000005002. Ann Surg. 2021. PMID: 34132695 Free PMC article. Clinical Trial.
-
The impact of prehospital TXA on mortality among bleeding trauma patients: A systematic review and meta-analysis.J Trauma Acute Care Surg. 2021 May 1;90(5):901-907. doi: 10.1097/TA.0000000000003120. J Trauma Acute Care Surg. 2021. PMID: 33605702
-
The Effectiveness of Prehospital Administration of Tranexamic Acid in Reducing Mortality in Trauma Patients: An Overview.Cureus. 2023 Dec 1;15(12):e49784. doi: 10.7759/cureus.49784. eCollection 2023 Dec. Cureus. 2023. PMID: 38161561 Free PMC article. Review.
Cited by
-
What you don't know can hurt you: a statistical commentary on missing data in trauma research.Trauma Surg Acute Care Open. 2024 Apr 2;9(1):e001405. doi: 10.1136/tsaco-2024-001405. eCollection 2024. Trauma Surg Acute Care Open. 2024. PMID: 38571726 Free PMC article. No abstract available.
-
Lost and found: how missing data connects TXA and outcomes in severely injured patients.Trauma Surg Acute Care Open. 2024 Mar 7;9(1):e001429. doi: 10.1136/tsaco-2024-001429. eCollection 2024. Trauma Surg Acute Care Open. 2024. PMID: 38464550 Free PMC article. No abstract available.
-
Early achievement of hemostasis defined by transfusion velocity: A possible mechanism for whole blood survival benefit.J Trauma Acute Care Surg. 2025 Mar 1;98(3):393-401. doi: 10.1097/TA.0000000000004507. Epub 2025 Jan 27. J Trauma Acute Care Surg. 2025. PMID: 39865522 Free PMC article.
References
-
- Cotton BA, Reddy N, Hatch QM, LeFebvre E, Wade CE, Kozar RA, Gill BS, Albarado R, McNutt MK, Holcomb JB. Damage control resuscitation is associated with a reduction in resuscitation volumes and improvement in survival in 390 damage control laparotomy patients. Ann Surg 2011;254:598–605. 10.1097/SLA.0b013e318230089e - DOI - PMC - PubMed
-
- Holcomb JB, del Junco DJ, Fox EE, Wade CE, Cohen MJ, Schreiber MA, Alarcon LH, Bai Y, Brasel KJ, Bulger EM, et al. . The prospective, observational, multicenter, major trauma transfusion (PROMMTT) study: comparative effectiveness of a time-varying treatment with competing risks. JAMA Surg 2013;148:127–36. 10.1001/2013.jamasurg.387 - DOI - PMC - PubMed
-
- Holcomb JB, Tilley BC, Baraniuk S, Fox EE, Wade CE, Podbielski JM, del Junco DJ, Brasel KJ, Bulger EM, Callcut RA, et al. . Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma: the PROPPR randomized clinical trial. JAMA 2015;313:471–82. 10.1001/jama.2015.12 - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials