

Pregnancy-associated mortality due to cardiovascular disease: Impact of hypertensive disorders of pregnancy
- PMID: 38375930
- PMCID: PMC10978238
- DOI: 10.1111/ppe.13055
Pregnancy-associated mortality due to cardiovascular disease: Impact of hypertensive disorders of pregnancy
Abstract
Background: Reported rates of maternal mortality in the United States have been staggeringly high and increasing, and cardiovascular disease (CVD) is a chief contributor to such deaths. However, the impact of hypertensive disorders of pregnancy (HDP) on the short-term risk of cardiovascular death is not well understood.
Objectives: To evaluate the association between HDP (chronic hypertension, gestational hypertension, preeclampsia, eclampsia, and superimposed preeclampsia) and pregnancy-associated mortality rates (PMR) from all causes, CVD-related causes both at delivery and within 1 year following delivery.
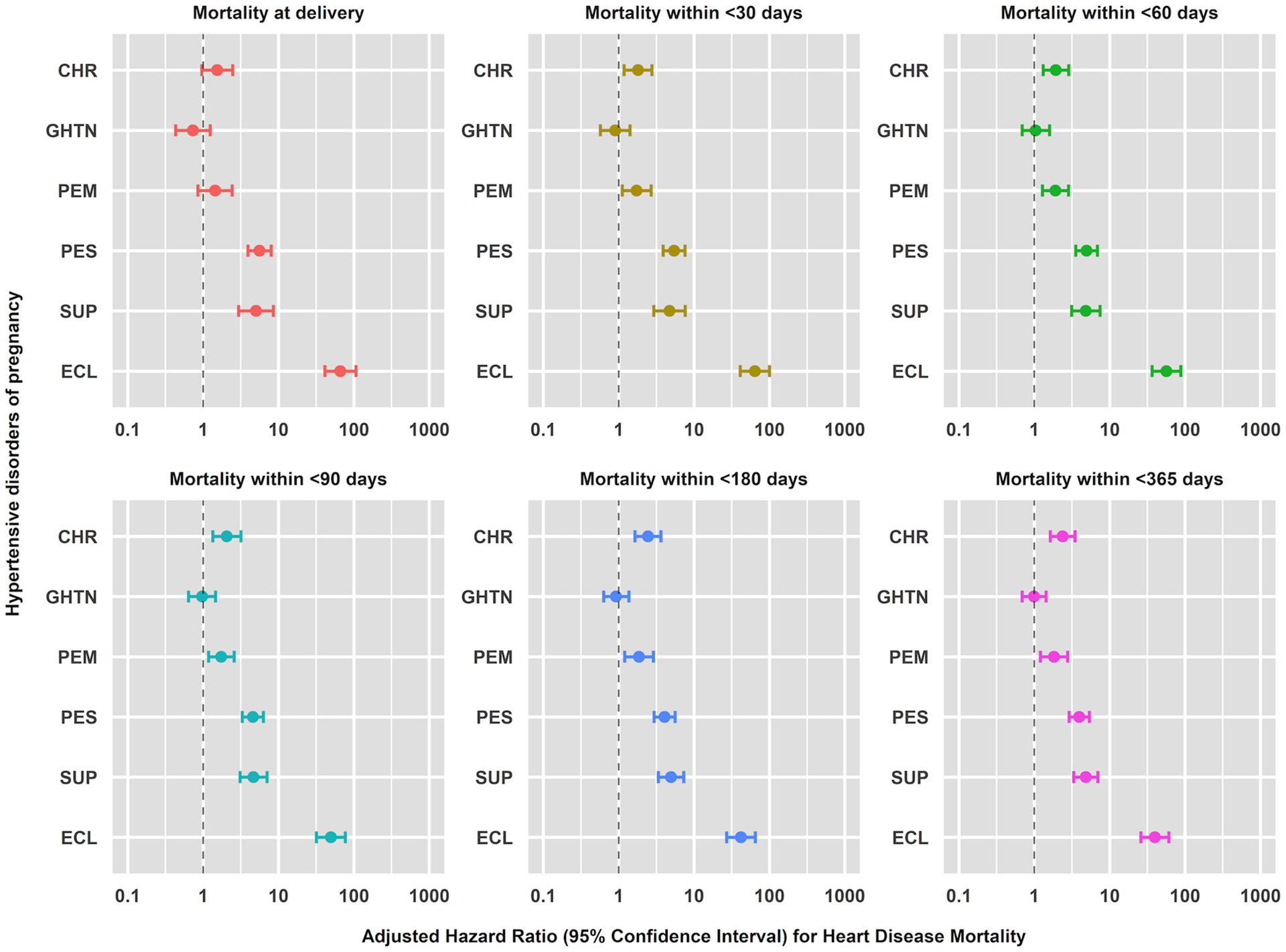
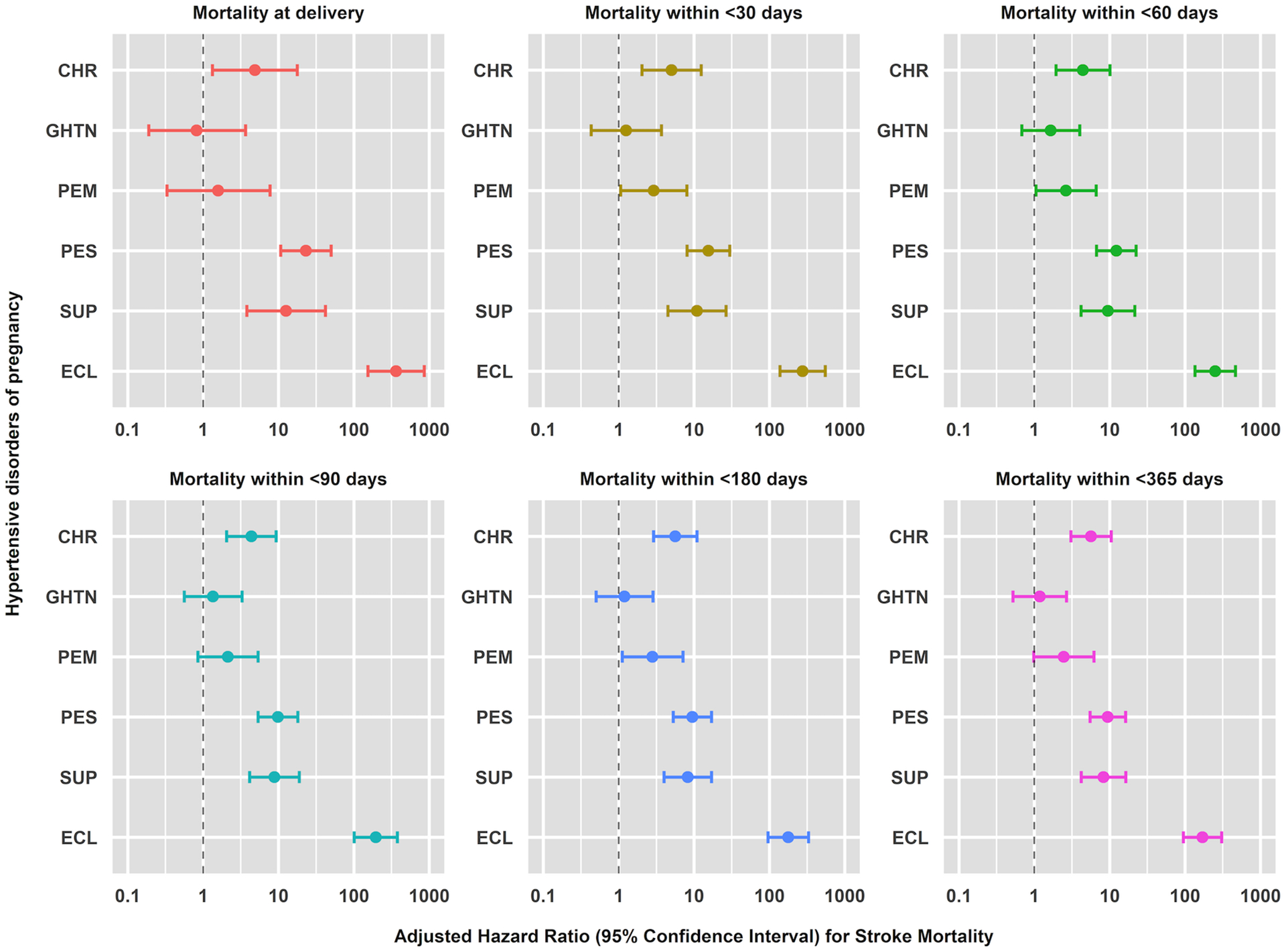
Methods: We used the Nationwide Readmissions Database (2010-2018) to examine PMRs for females 15-54 years old. International Classification of Disease 9 and 10 diagnosis codes were used to identify pregnancy-associated deaths due to HDP and CVD. Discrete-time Cox proportional hazards regression models were used to calculate adjusted hazard ratios (HR) and 95% confidence intervals (CI) for mortality at delivery (0 days) and at <30, <60, <90, <180, and <365 days after delivery in relation to HDP.
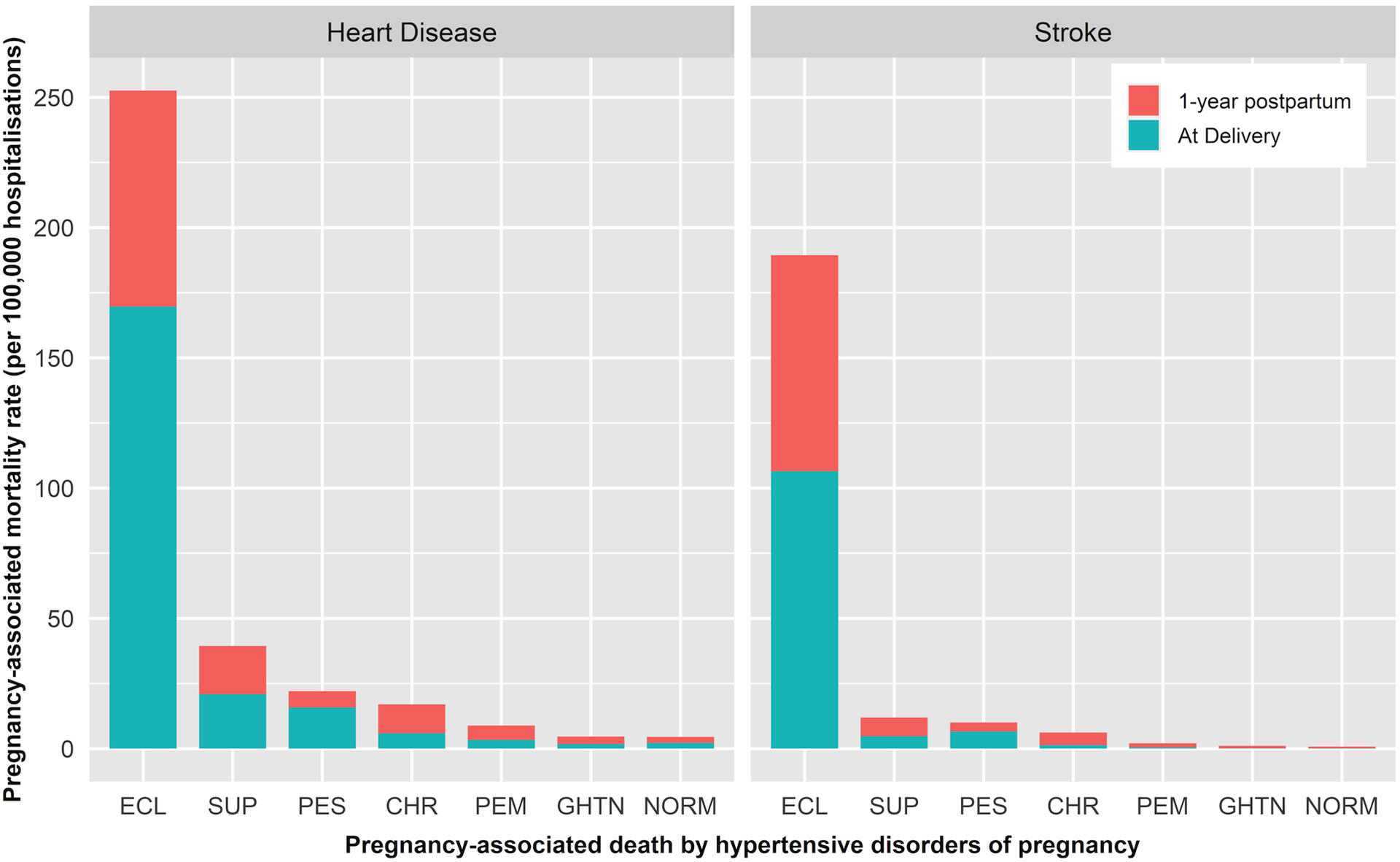
Results: Of 33,417,736 hospital deliveries, the rate of HDP was 11.0% (n = 3,688,967), and the PMR from CVD was 6.4 per 100,000 delivery hospitalisations (n = 2141). Compared with normotensive patients, HRs for CVD-related PMRs increased with HDP severity, reaching over 58-fold for eclampsia patients. HRs were higher for stroke-related (1.2 to 170.9) than heart disease (HD)-related (0.99 to 39.8) mortality across all HDPs. Except for gestational hypertension, the increased risks of CVD mortality were evident at delivery and persisted 1 year postpartum for all HDPs.
Conclusions: HDPs are strong risk factors for pregnancy-associated mortality due to CVD at delivery and within 1 year postpartum; the risks are stronger for stroke than HD-related PMR. While absolute PMRs are low, this study supports the importance of extending postpartum care beyond the traditional 42-day postpartum visit for people whose pregnancies are complicated by hypertension.
Keywords: cardiovascular disease; heart disease; hypertensive disorders of pregnancy; pregnancy‐associated mortality; stroke.
© 2024 The Authors. Paediatric and Perinatal Epidemiology published by John Wiley & Sons Ltd.
Figures
References
-
- Hoyert DL. Maternal mortality rates in the United States, 2021. NCHS Health E-Stats. 2023. doi: DOI: 10.15620/cdc:124678. - DOI
-
- Declercq E, Zephyrin L. Maternal Mortality in the United States: A Primer. 2020.
-
- Hoyert DL, Minino AM. Maternal Mortality in the United States: Changes in Coding, Publication, and Data Release, 2018. Natl Vital Stat Rep. 2020;69:1–18. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
