

Viral and Host Factors Are Associated With Mortality in Hospitalized Patients With COVID-19
- PMID: 38376212
- PMCID: PMC11175705
- DOI: 10.1093/cid/ciad780
Viral and Host Factors Are Associated With Mortality in Hospitalized Patients With COVID-19
Abstract
Background: Persistent mortality in adults hospitalized due to acute COVID-19 justifies pursuit of disease mechanisms and potential therapies. The aim was to evaluate which virus and host response factors were associated with mortality risk among participants in Therapeutics for Inpatients with COVID-19 (TICO/ACTIV-3) trials.
Methods: A secondary analysis of 2625 adults hospitalized for acute SARS-CoV-2 infection randomized to 1 of 5 antiviral products or matched placebo in 114 centers on 4 continents. Uniform, site-level collection of participant baseline clinical variables was performed. Research laboratories assayed baseline upper respiratory swabs for SARS-CoV-2 viral RNA and plasma for anti-SARS-CoV-2 antibodies, SARS-CoV-2 nucleocapsid antigen (viral Ag), and interleukin-6 (IL-6). Associations between factors and time to mortality by 90 days were assessed using univariate and multivariable Cox proportional hazards models.
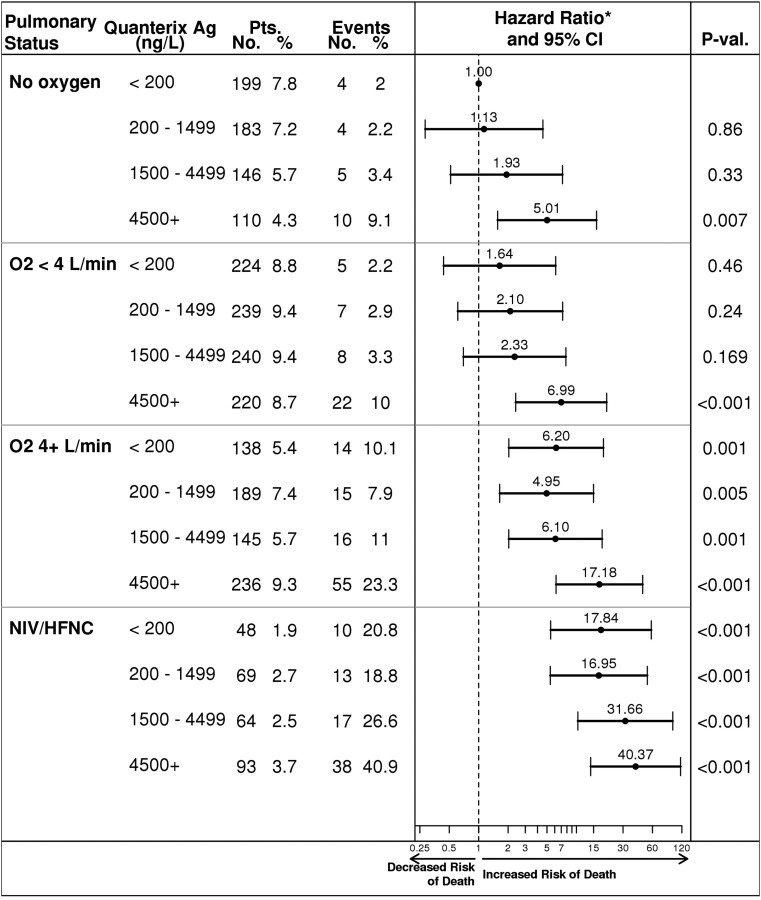
Results: Viral Ag ≥4500 ng/L (vs <200 ng/L; adjusted hazard ratio [aHR], 2.07; 1.29-3.34), viral RNA (<35 000 copies/mL [aHR, 2.42; 1.09-5.34], ≥35 000 copies/mL [aHR, 2.84; 1.29-6.28], vs below detection), respiratory support (<4 L O2 [aHR, 1.84; 1.06-3.22]; ≥4 L O2 [aHR, 4.41; 2.63-7.39], or noninvasive ventilation/high-flow nasal cannula [aHR, 11.30; 6.46-19.75] vs no oxygen), renal impairment (aHR, 1.77; 1.29-2.42), and IL-6 >5.8 ng/L (aHR, 2.54 [1.74-3.70] vs ≤5.8 ng/L) were significantly associated with mortality risk in final adjusted analyses. Viral Ag, viral RNA, and IL-6 were not measured in real-time.
Conclusions: Baseline virus-specific, clinical, and biological variables are strongly associated with mortality risk within 90 days, revealing potential pathogen and host-response therapeutic targets for acute COVID-19 disease.
Keywords: acute COVID-19; host response; viral factors.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Potential conflicts of interest. N. R. A. reports support for attending meetings and/or travel to their institution from the National Institutes of Health (NIH). D. L. B. reports consulting fees and payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events, and participation on a Data Safety Monitoring Board (DSMB) or Advisory Board with Pfizer, Gilead, MSD, and ViiV; and support for attending meetings and/or travel from ViiV and Gilead. M. K. J. reports a grant to their institution from Gilead Sciences and a contract for a clinical trial to their institution from Regeneron; and a role on the HIV MA Board of Directors. J. P. H. reports consulting fees to the author from Pfizer, MSD, Menarini, Angelini, Zambon, and Tillots; payment or honoraria payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events to their institution and the author from Pfizer and to the author from MSD and Angelini; support for attending meetings and/or travel from MSD and Pfizer; and paid participation as a DSMB member for a TFT Pharmaceuticals clinical trial. K. K. reports grants or contracts to their institution from the NIH, COVID Vaccine Prevention Network, (NIH), Regeneron, Abbott, Pfizer, Romark, and Raisonance; royalties or licenses to book author for Elsevier; consulting fees to the author from Regeneron; payment for expert testimony to the author from the State of Florida; support for travel from Sanford Guide, Burroughs Wellcome Fund, ParaFrap, and the Infectious Diseases Society of America (IDSA) Board of Directors; patents planned, issued, or pending to University of South Florida (USF) F and USF faculty from 3D swabs; leadership or a fiduciary role on the Sanford Guide, Burroughs Wellcome Fund, IDSA board, and ParaFrap; and personal stocks from Gilead. S. L. P. reports grants paid to the University College London, which are completely separate from this work, with Medical Research Council, United Kingdom Research and Innovation, The European and Developing Countries Clinical Trial Partnership, Janssen-Cilag, Gilead Sciences, and ViiV Healthcare; participation as member of the DSMB for the TIPAL trial (The effectiveness and risks of Treating people with Idiopathic Pulmonary fibrosis with the Addition of Lansoprazole: a randomized placebo-controlled multicenter clinical trial). This is an academic trial funded in the United Kingdom by the National Institute for Health and Care Research (NIHR), UK. C. R. reports grants or contracts from NIH and participation on a DSMB or Advisory Board from Mayo Clinic and NIH. U. S. reports research grants or contracts from ViiV Healthcare and AstraZeneca; consulting fees from Shionogi, Paratek, ViiV, and Pfizer; and payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Shionogi, Pfizer, and Paratek. B. W. T. reports grants or contracts from Veterans Affairs (VA) Health Services and Development Service Center for Innovations in Quality, Effectiveness, and Safety (13-413), Agency for Healthcare Research and Quality (AHRQ), VA Rehabilitation Research and Development, and Peptilogics; consulting fees from Phiogen; and payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from the George Washington ID Board Review Course, the Warren Alpert Medical School of Brown University. A. A. G. reports grants to their institution from Centers for Disease Control, Department of Defense, Faron Pharmaceuticals, and AbbVie; participation on a DSMB or Advisory Board from NIH; and a role on the Scientific Advisory Board from Biomeme. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
Comment in
-
Viral, Host Factors or Both as COVID-19 Biomarkers.Clin Infect Dis. 2024 Jun 14;78(6):1504-1505. doi: 10.1093/cid/ciad779. Clin Infect Dis. 2024. PMID: 38376208 No abstract available.
References
-
- Kim L, Garg S, O'Halloran A, et al. Risk factors for intensive care unit admission and in-hospital mortality among hospitalized adults identified through the US coronavirus disease 2019 (COVID-19)-associated Hospitalization Surveillance Network (COVID-NET). Clin Infect Dis 2021; 72:e206–e14. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
