

A population pharmacokinetic model for posaconazole intravenous solution and oral powder for suspension formulations in pediatric patients with neutropenia
- PMID: 38376229
- PMCID: PMC10994819
- DOI: 10.1128/aac.01197-23
A population pharmacokinetic model for posaconazole intravenous solution and oral powder for suspension formulations in pediatric patients with neutropenia
Abstract
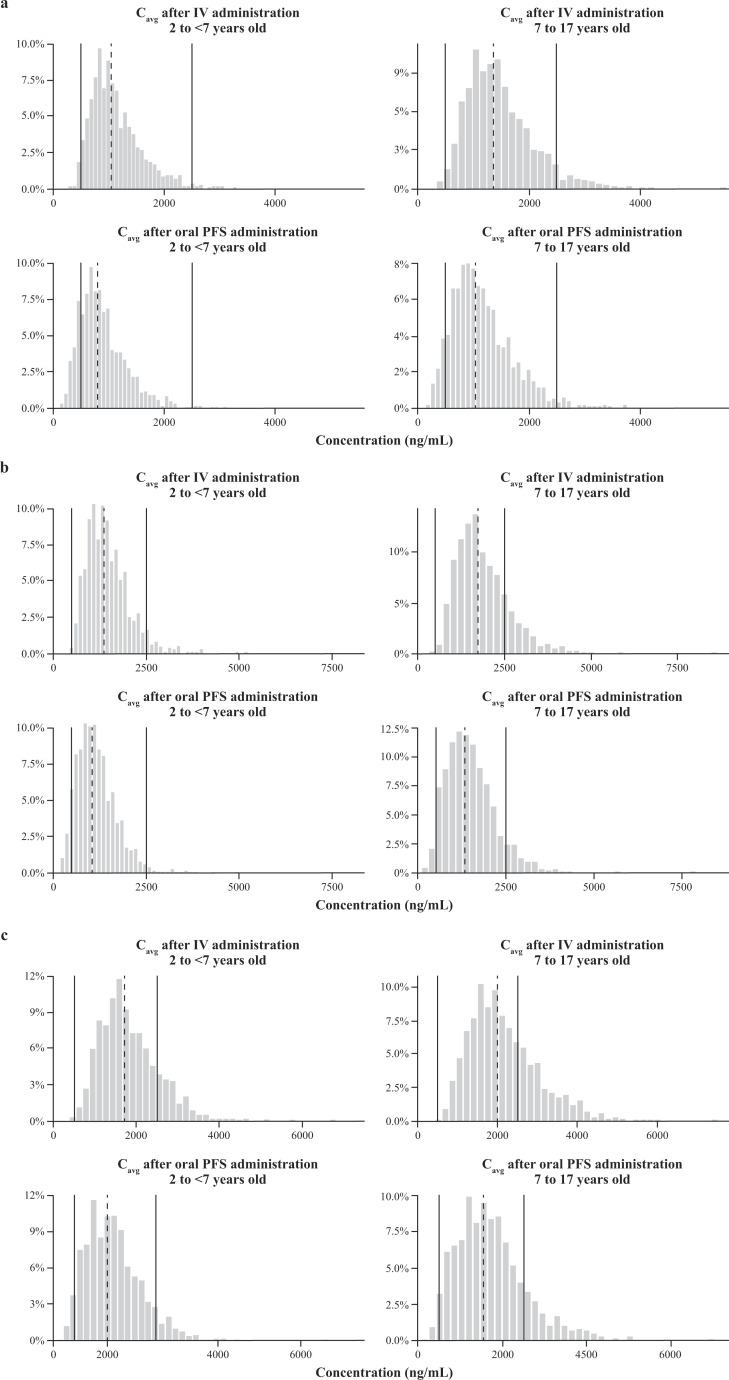
The objective of this study was to support posaconazole dose regimens in pediatric patients aged ≥2 years, using a population pharmacokinetic (PK) approach with data from a phase 1b study (NCT02452034). A one-compartment model with first-order absorption was fit to pharmacokinetic data from 144 participants aged 2 to 17 years, who were administered posaconazole as intravenous (IV) and powder for oral suspension (PFS) formulations, or IV only, at dosing regimens of 3.5, 4.5, and 6 mg/kg. The influence of demographic and clinical factors on pharmacokinetic parameters was evaluated using a stepwise forward inclusion/backward exclusion procedure. The final model simulated posaconazole exposure in patients aged 2 to <7 and 7 to 17 years at dosing regimens of 4.5, 6, and 7.5 mg/kg. Plasma concentration data following IV and PFS administration were well-described by a one-compartment model with first-order absorption and estimated bioavailability, where clearance and volume were subject to allometric scaling by body weight. The 6-mg/kg dosing regimen achieved the pharmacokinetic target (90% of the pediatric population having an average steady-state plasma concentration of ≥500 and <2,000 ng/mL) for both age groups, regardless of whether patients received IV and PFS or IV only. In a virtual adolescent population (body weight >40 kg), the 300 mg/day posaconazole tablet was also predicted to achieve the pharmacokinetic target and remain within a safe range of exposure. These data informed a weight-based nomogram for PFS dosing to maximize the number of pediatric patients achieving the pharmacokinetic target across weight bands, while also maintaining a favorable benefit/risk profile.
Keywords: antifungal agents; invasive fungal disease; pediatrics; pharmacokinetics; posaconazole.
Conflict of interest statement
R.W., E.M., C.B., and H.W. are current or former employees of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA, and may own stock and/or options in Merck & Co., Inc., Rahway, NJ, USA. R.G. owns stock and/or options in Merck & Co., Inc., Rahway, NJ, USA. A.O., R.G., and G.W. received consulting fees paid to Certara by Merck for contribution. A.O., R.G., F.F., G.W., R.W., C.B., E.M., and H.W. have no conflicts to report.
Figures



References
-
- De Pauw B, Walsh TJ, Donnelly JP, Stevens DA, Edwards JE, Calandra T, Pappas PG, Maertens J, Lortholary O, Kauffman CA, et al. . 2008. Revised definitions of invasive fungal disease from the European organization for research and treatment of cancer/invasive fungal infections cooperative group and the national institute of allergy and infectious diseases mycoses study group (EORTC/MSG) consensus group. Clin Infect Dis 46:1813–1821. doi:10.1086/588660 - DOI - PMC - PubMed
-
- Castagnola E, Cesaro S, Giacchino M, Livadiotti S, Tucci F, Zanazzo G, Caselli D, Caviglia I, Parodi S, Rondelli R, Cornelli PE, Mura R, Santoro N, Russo G, De Santis R, Buffardi S, Viscoli C, Haupt R, Rossi MR. 2006. Fungal infections in children with cancer: a prospective, multicenter surveillance study. Pediatr Infect Dis J 25:634–639. doi:10.1097/01.inf.0000220256.69385.2e - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
