

Automated vessel-specific coronary artery calcification quantification with deep learning in a large multi-centre registry
- PMID: 38376471
- PMCID: PMC11210989
- DOI: 10.1093/ehjci/jeae045
Automated vessel-specific coronary artery calcification quantification with deep learning in a large multi-centre registry
Abstract
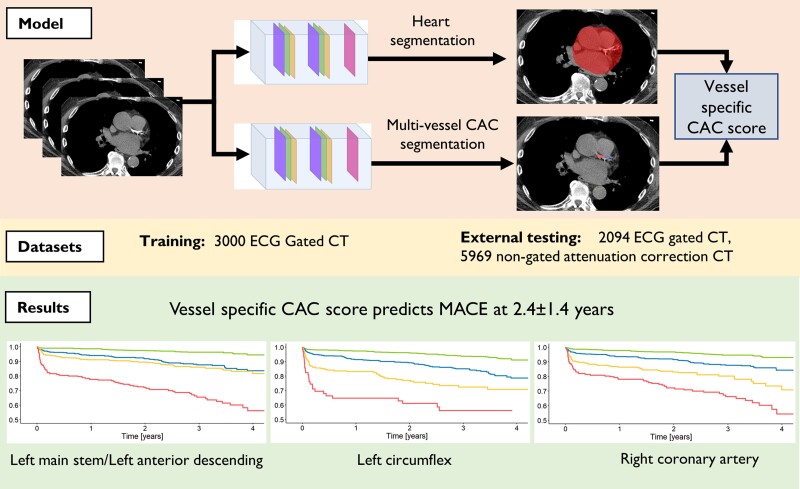
Aims: Vessel-specific coronary artery calcification (CAC) is additive to global CAC for prognostic assessment. We assessed accuracy and prognostic implications of vessel-specific automated deep learning (DL) CAC analysis on electrocardiogram (ECG) gated and attenuation correction (AC) computed tomography (CT) in a large multi-centre registry.
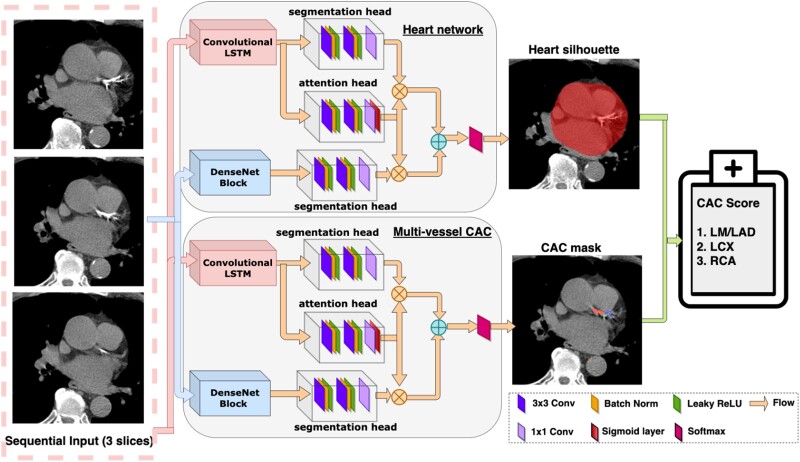
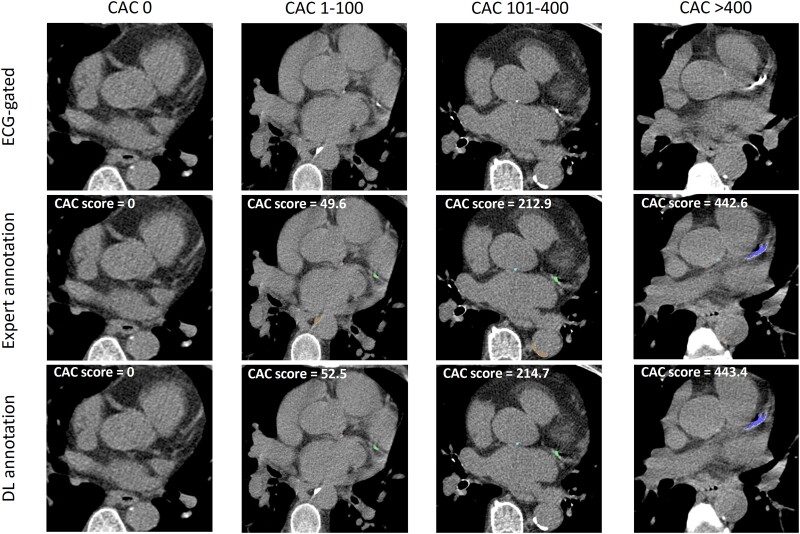
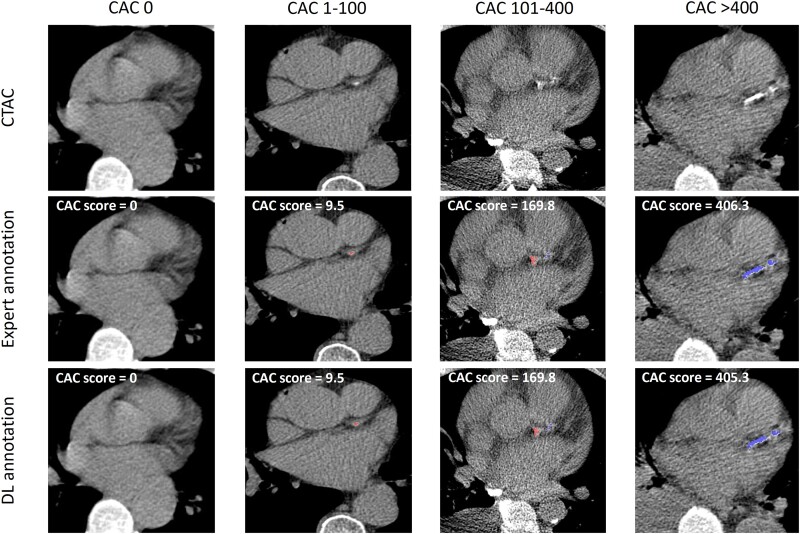
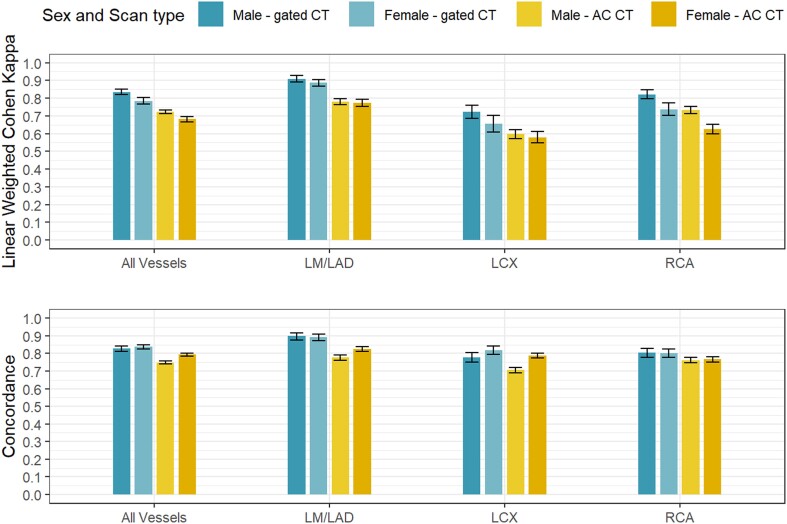
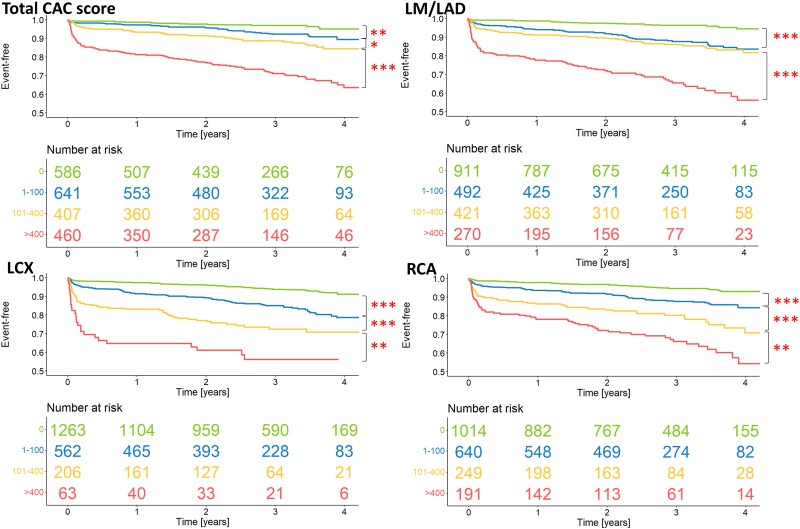
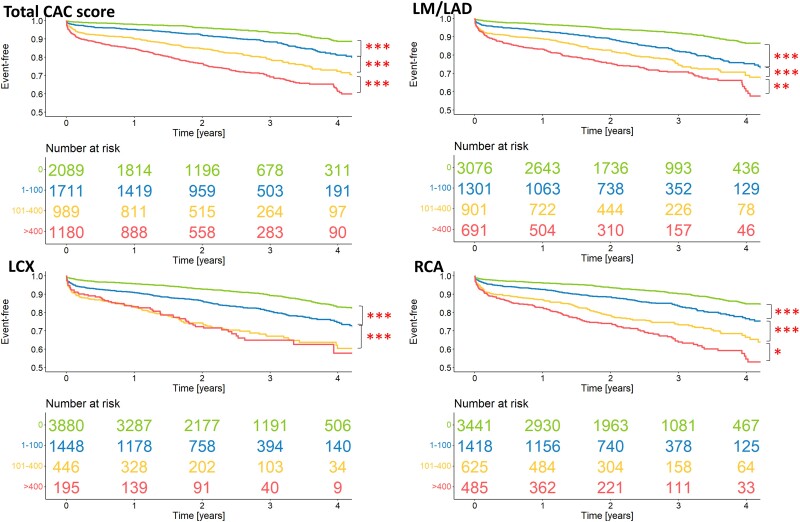
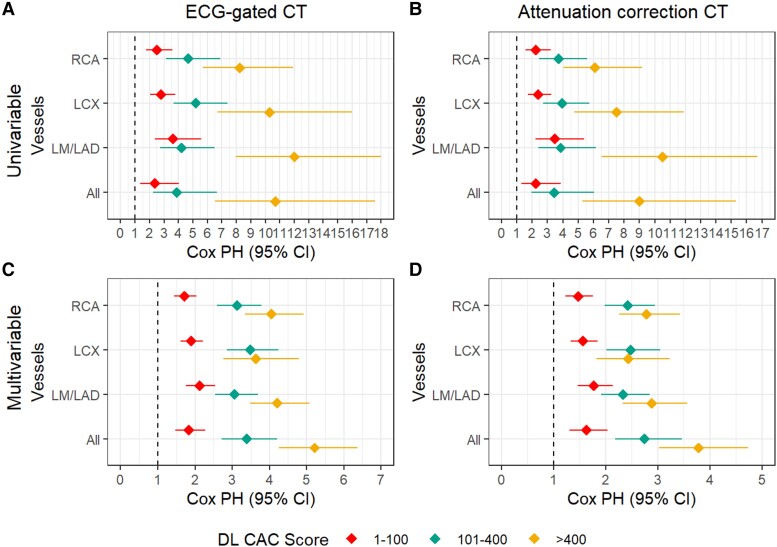
Methods and results: Vessel-specific CAC was assessed in the left main/left anterior descending (LM/LAD), left circumflex (LCX), and right coronary artery (RCA) using a DL model trained on 3000 gated CT and tested on 2094 gated CT and 5969 non-gated AC CT. Vessel-specific agreement was assessed with linear weighted Cohen's Kappa for CAC zero, 1-100, 101-400, and >400 Agatston units (AU). Risk of major adverse cardiovascular events (MACE) was assessed during 2.4 ± 1.4 years follow-up, with hazard ratios (HR) and 95% confidence intervals (CI). There was strong to excellent agreement between DL and expert ground truth for CAC in LM/LAD, LCX and RCA on gated CT [0.90 (95% CI 0.89 to 0.92); 0.70 (0.68 to 0.73); 0.79 (0.77 to 0.81)] and AC CT [0.78 (0.77 to 0.80); 0.60 (0.58 to 0.62); 0.70 (0.68 to 0.71)]. MACE occurred in 242 (12%) undergoing gated CT and 841(14%) of undergoing AC CT. LM/LAD CAC >400 AU was associated with the highest risk of MACE on gated (HR 12.0, 95% CI 7.96, 18.0, P < 0.001) and AC CT (HR 4.21, 95% CI 3.48, 5.08, P < 0.001).
Conclusion: Vessel-specific CAC assessment with DL can be performed accurately and rapidly on gated CT and AC CT and provides important prognostic information.
Keywords: computed tomography; coronary artery calcification; coronary artery disease; deep learning.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology. All rights reserved. For commercial re-use, please contact reprints@oup.com for reprints and translation rights for reprints. All other permissions can be obtained through our RightsLink service via the Permissions link on the article page on our site—for further information please contact journals.permissions@oup.com.
Conflict of interest statement
Conflict of interest: M.C.W. has given talks for Canon Medical Systems and Siemens Healthineers. Dr. Robert Miller has received consulting fees and research support from Pfizer. Drs. Berman and Slomka and Mr. Kavanagh participate in software royalties for QPS software at Cedars-Sinai Medical Center. Dr. Berman is a consultant for GE Healthcare and Dr. Edward Miller has served as Pfizer, Eidos, CSL Behring, Anylam, and GE Healthcare consultant with grant support from Eidos, Pfizer, and Anylam. Dr. Slomka has received research grant support from Siemens Medical Systems. The remaining authors have no relevant disclosures.
Figures
References
-
- WHO . Cardiovascular diseases (CVDs) 2021 [updated 16 August 2021; cited 2021 16 August 2021]. Available from: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases....
-
- Williams MC, Moss A, Dweck M, Hunter A, Pawade T, Adamson PDet al. Standardized reporting systems for computed tomography coronary angiography and calcium scoring: a real-world validation of CAD-RADS and CAC-DRS in patients with stable chest pain. J Cardiovasc Comput Tomogr 2020;14:3–11. - PubMed
-
- Detrano R, Guerci AD, Carr JJ, Bild DE, Burke G, Folsom ARet al. Coronary calcium as a predictor of coronary events in four racial or ethnic groups. N Engl J Med 2008;358:1336–45. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
