Early systemic insults following traumatic brain injury: association with biomarker profiles, therapy for intracranial hypertension, and neurological outcomes-an analysis of CENTER-TBI data
- PMID: 38376517
- PMCID: PMC10955000
- DOI: 10.1007/s00134-024-07324-8
Early systemic insults following traumatic brain injury: association with biomarker profiles, therapy for intracranial hypertension, and neurological outcomes-an analysis of CENTER-TBI data
Abstract
Purpose: We analysed the impact of early systemic insults (hypoxemia and hypotension, SIs) on brain injury biomarker profiles, acute care requirements during intensive care unit (ICU) stay, and 6-month outcomes in patients with traumatic brain injury (TBI).
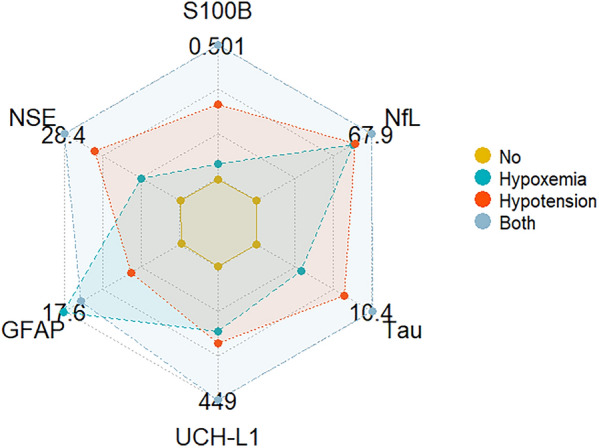
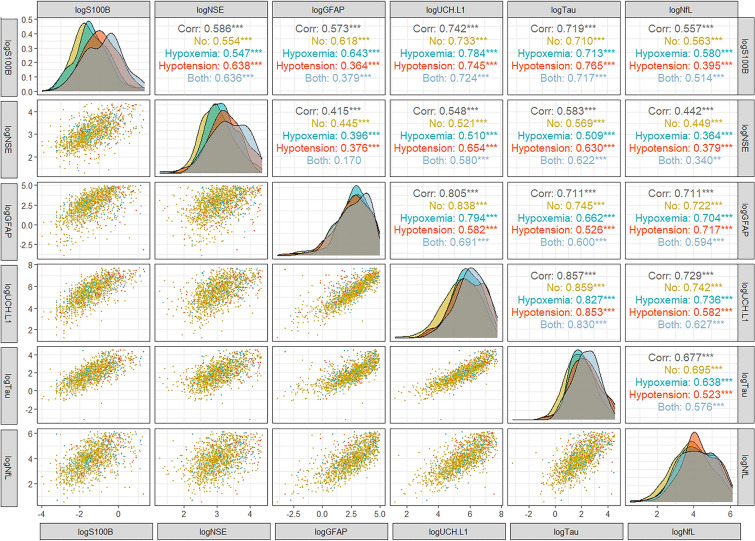
Methods: From patients recruited to the Collaborative European neurotrauma effectiveness research in TBI (CENTER-TBI) study, we documented the prevalence and risk factors for SIs and analysed their effect on the levels of brain injury biomarkers [S100 calcium-binding protein B (S100B), neuron-specific enolase (NSE), neurofilament light (NfL), glial fibrillary acidic protein (GFAP), ubiquitin carboxy-terminal hydrolase L1 (UCH-L1), and protein Tau], critical care needs, and 6-month outcomes [Glasgow Outcome Scale Extended (GOSE)].
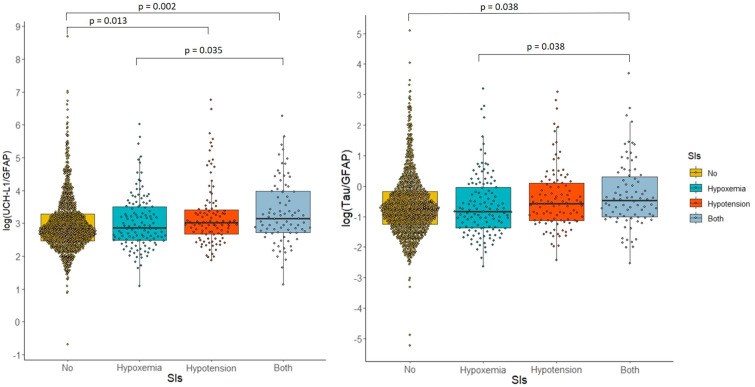
Results: Among 1695 TBI patients, 24.5% had SIs: 16.1% had hypoxemia, 15.2% had hypotension, and 6.8% had both. Biomarkers differed by SI category, with higher S100B, Tau, UCH-L1, NSE and NfL values in patients with hypotension or both SIs. The ratio of neural to glial injury (quantified as UCH-L1/GFAP and Tau/GFAP ratios) was higher in patients with hypotension than in those with no SIs or hypoxia alone. At 6 months, 380 patients died (22%), and 759 (45%) had GOSE ≤ 4. Patients who experienced at least one SI had higher mortality than those who did not (31.8% vs. 19%, p < 0.001).
Conclusion: Though less frequent than previously described, SIs in TBI patients are associated with higher release of neuronal than glial injury biomarkers and with increased requirements for ICU therapies aimed at reducing intracranial hypertension. Hypotension or combined SIs are significantly associated with adverse 6-month outcomes. Current criteria for hypotension may lead to higher biomarker levels and more negative outcomes than those for hypoxemia suggesting a need to revisit pressure targets in the prehospital settings.
Keywords: Hypotension; Hypoxemia; Outcome; Serum biomarkers; Systemic insults; Traumatic brain injury.
© 2024. The Author(s).
Conflict of interest statement
GC reports grants and personal fees as a speakers' bureau member and advisory board member from Integra Neurosciences, NeurOptics, Biogen, Invex Ltd and Idorsia, all outside the submitted work. DKM reports consultancy fees, speaker fees, or research collaborations with NeuroTrauma Sciences, Lantmannen AB, GlaxoSmithKline Ltd, Pressura Neuro Ltd, Integra Neurosciences, and Invex Ltd. CR reports speaker fees from Edwards Life Sciences and Masimo. The other authors did not declare competing interests.
Figures