

Task force of the Brazilian Society of Otology - evaluation and management of peripheral facial palsy
- PMID: 38377729
- PMCID: PMC10884764
- DOI: 10.1016/j.bjorl.2023.101374
Task force of the Brazilian Society of Otology - evaluation and management of peripheral facial palsy
Abstract
Objective: To review key evidence-based recommendations for the diagnosis and treatment of peripheral facial palsy in children and adults.
Methods: Task force members were educated on knowledge synthesis methods, including electronic database search, review and selection of relevant citations, and critical appraisal of selected studies. Articles written in English or Portuguese on peripheral facial palsy were eligible for inclusion. The American College of Physicians' guideline grading system and the American Thyroid Association's guideline criteria were used for critical appraisal of evidence and recommendations for therapeutic interventions.
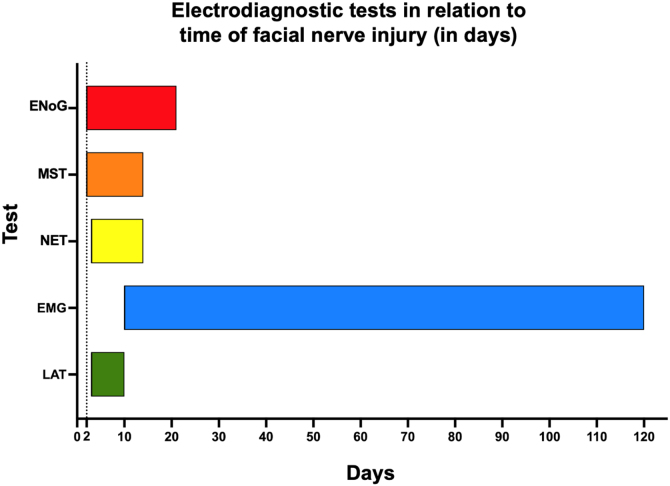
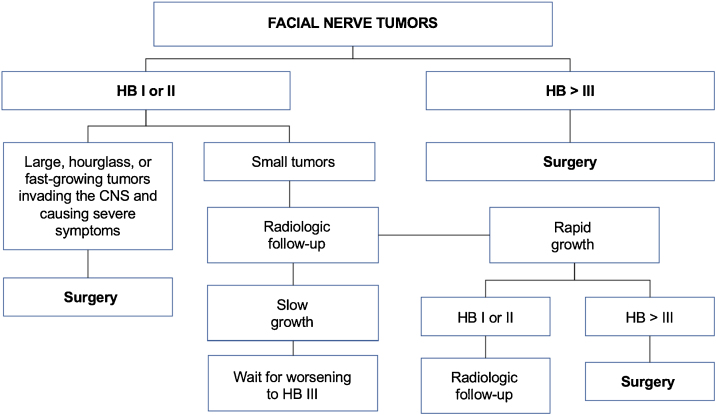
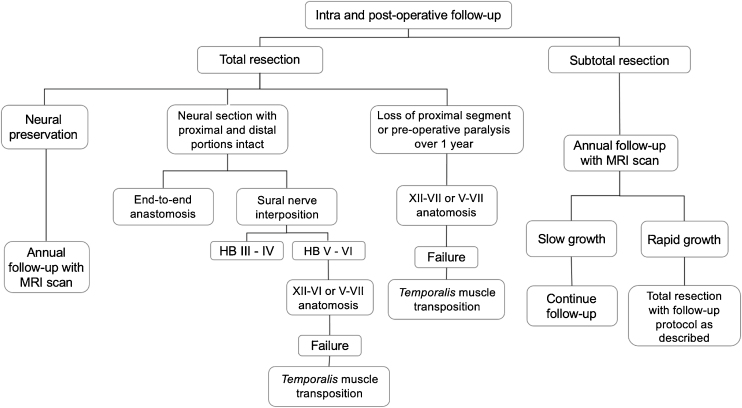
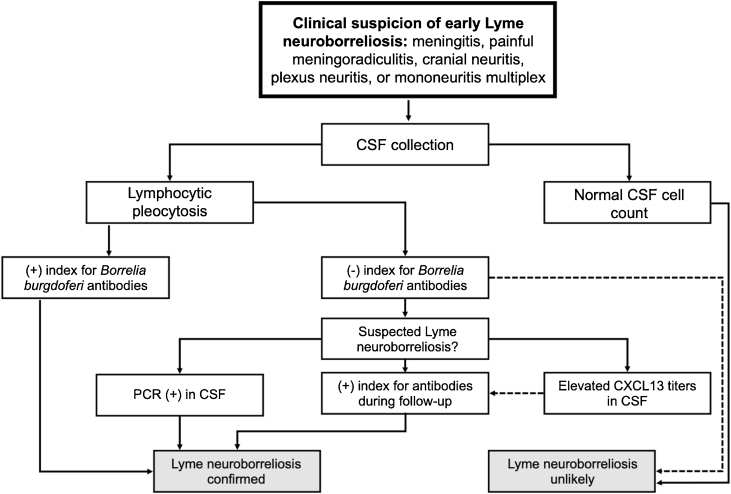
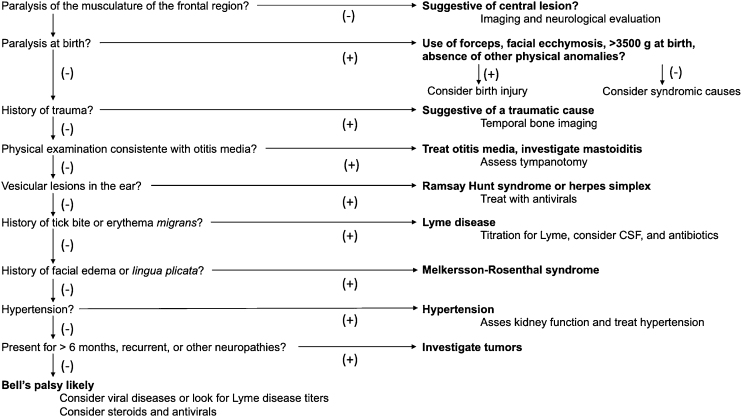
Results: The topics were divided into 2 main parts: (1) Evaluation and diagnosis of facial palsy: electrophysiologic tests, idiopathic facial palsy, Ramsay Hunt syndrome, traumatic peripheral facial palsy, recurrent peripheral facial palsy, facial nerve tumors, and peripheral facial palsy in children; and (2) Rehabilitation procedures: surgical decompression of the facial nerve, facial nerve grafting, surgical treatment of long-term peripheral facial palsy, and non-surgical rehabilitation of the facial nerve.
Conclusions: Peripheral facial palsy is a condition of diverse etiology. Treatment should be individualized according to the cause of facial nerve dysfunction, but the literature presents better evidence-based recommendations for systemic corticosteroid therapy.
Keywords: Bell palsy; Facial nerve disease; Facial nerve trauma; Facial palsy; Facial paralysis; Guidelines; Herpes Zoster Oticus; Microvascular decompression surgery.
Copyright © 2023. Published by Elsevier España S.L.U.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
