

Percutaneous transforaminal endoscopic decompression with removal of the posterosuperior region underneath the slipping vertebral body for lumbar spinal stenosis with degenerative lumbar spondylolisthesis: a retrospective study
- PMID: 38378495
- PMCID: PMC10877792
- DOI: 10.1186/s12891-024-07267-7
Percutaneous transforaminal endoscopic decompression with removal of the posterosuperior region underneath the slipping vertebral body for lumbar spinal stenosis with degenerative lumbar spondylolisthesis: a retrospective study
Abstract
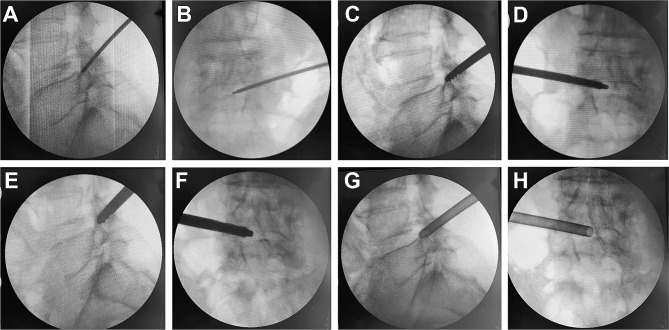
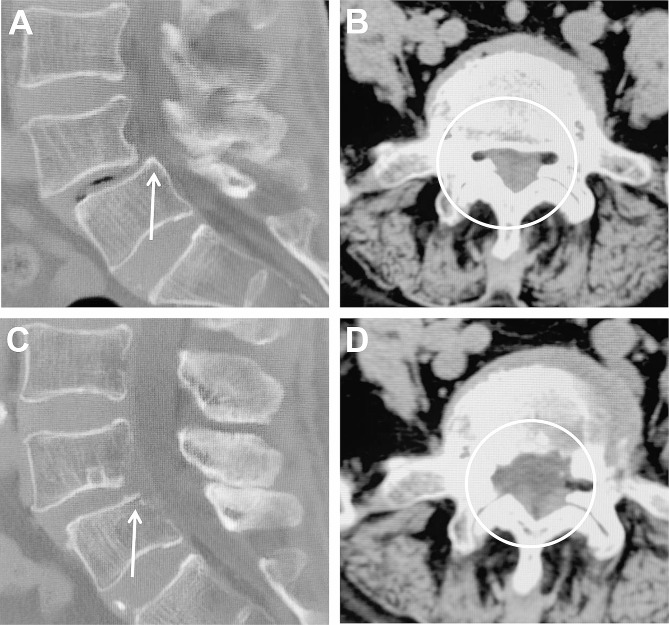
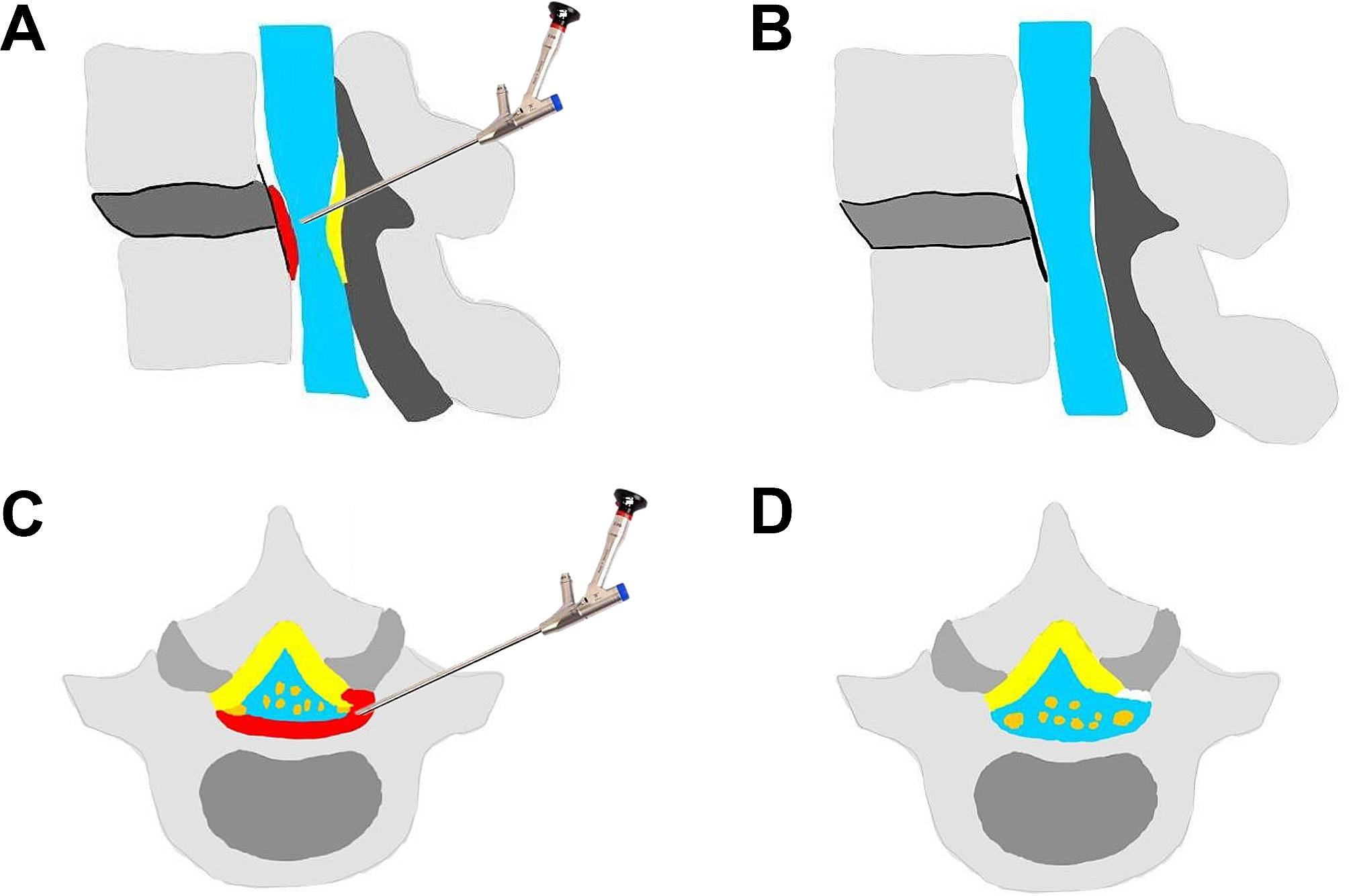
Background: Percutaneous transforaminal endoscopic decompression (PTED) is an ideal minimally invasive decompression technique for the treatment of lumbar spinal stenosis (LSS) with degenerative lumbar spondylolisthesis (DLS). The posterosuperior region underneath the slipping vertebral body (PRSVB) formed by DLS is an important factor exacerbating LSS in patients. Therefore, the necessity of removing the PRSVB during ventral decompression remains to be discussed. This study aimed to describe the procedure of PTED combined with the removal of the PRSVB and to evaluate the clinical outcomes.
Methods: LSS with DLS was diagnosed in 44 consecutive patients at our institution from January 2019 to July 2021, and they underwent PTED combined with the removal of the PRSVB. All patients were followed up for at least 12 months. The clinical outcomes were evaluated using the visual analog scale (VAS), Oswestry Disability Index (ODI), and modified MacNab criteria.
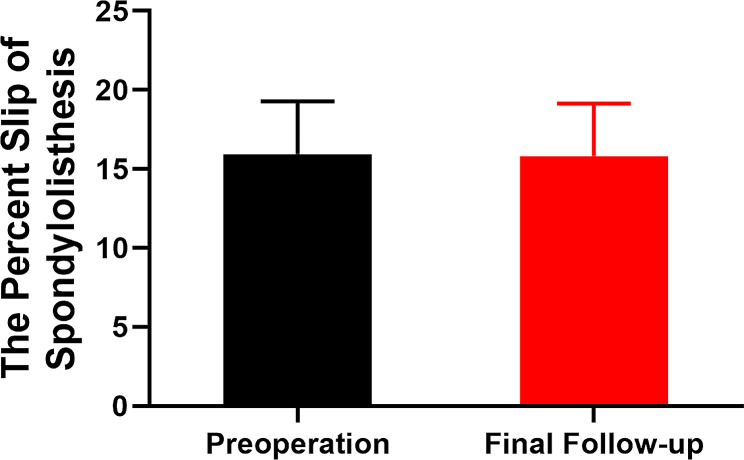
Results: The mean age of the patients was 69.5 ± 7.1 years. The mean preoperative ODI score, VAS score of the low back, and VAS score of the leg were 68.3 ± 10.8, 5.8 ± 1.0, and 7.7 ± 1.1, respectively, which improved to 18.8 ± 5.0, 1.4 ± 0.8, and 1.6 ± 0.7, respectively, at 12 months postoperatively. The proportion of patients presenting "good" and "excellent" ratings according to the modified MacNab criteria was 93.2%. The percent slippage in spondylolisthesis preoperatively (16.0% ± 3.3%) and at the end of follow-up (15.8% ± 3.3%) did not differ significantly (p>0.05). One patient had a dural tear, and one patient had postoperative dysesthesia.
Conclusions: Increasing the removal of PRSVB during the PTED process may be a beneficial surgical procedure for alleviating clinical symptoms in patients with LSS and DLS. However, long-term follow-up is needed to study clinical effects.
Keywords: Bone drill; Degenerative lumbar spondylolisthesis; Local anesthesia; Lumbar spinal stenosis; Percutaneous transforaminal endoscopic decompression; Posterosuperior region underneath the slipping vertebral body.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



Similar articles
-
Endoscopic Ventral Decompression for Spinal Stenosis with Degenerative Spondylolisthesis by Partially Removing Posterosuperior Margin Underneath the Slipping Vertebral Body: Technical Note and Outcome Evaluation.World Neurosurg. 2019 Jun;126:e517-e525. doi: 10.1016/j.wneu.2019.02.083. Epub 2019 Feb 28. World Neurosurg. 2019. PMID: 30825627
-
Percutaneous transforaminal endoscopic decompression for lumbar spinal stenosis with degenerative spondylolisthesis in the elderly.Clin Neurol Neurosurg. 2020 Jul;194:105918. doi: 10.1016/j.clineuro.2020.105918. Epub 2020 May 16. Clin Neurol Neurosurg. 2020. PMID: 32446122
-
Comparison of 270-degree percutaneous transforaminal endoscopic decompression under local anesthesia and minimally invasive transforaminal lumbar interbody fusion in the treatment of geriatric lateral recess stenosis associated with degenerative lumbar spondylolisthesis.J Orthop Surg Res. 2023 Mar 9;18(1):183. doi: 10.1186/s13018-023-03676-x. J Orthop Surg Res. 2023. PMID: 36895012 Free PMC article.
-
[Surgical Treatment of Degenerative Lumbar Stenosis and Spondylolisthesis: Clinical Practice Guideline].Acta Chir Orthop Traumatol Cech. 2023;90(3):157-167. Acta Chir Orthop Traumatol Cech. 2023. PMID: 37395422 Czech.
-
Does Concomitant Degenerative Spondylolisthesis Influence the Outcome of Decompression Alone in Degenerative Lumbar Spinal Stenosis? A Meta-Analysis of Comparative Studies.World Neurosurg. 2019 Mar;123:226-238. doi: 10.1016/j.wneu.2018.11.246. Epub 2018 Dec 18. World Neurosurg. 2019. PMID: 30576810 Review.
Cited by
-
Percutaneous transforaminal endoscopic decompression versus posterior short-segment fusion for treating degenerative lumbar scoliosis with lumbar spinal stenosis: a cohort study with a minimum five year followup.Int Orthop. 2025 May;49(5):1211-1222. doi: 10.1007/s00264-025-06479-3. Epub 2025 Mar 10. Int Orthop. 2025. PMID: 40063116
-
Percutaneous Transforaminal Endoscopic Lumbar Foraminotomy in Stable Degenerative Lumbar Isthmic Spondylolisthesis with Radicular Leg Pain: A Retrospective Study.J Pain Res. 2024 May 28;17:1953-1965. doi: 10.2147/JPR.S454771. eCollection 2024. J Pain Res. 2024. PMID: 38828087 Free PMC article.
-
Advancements in Spinal Endoscopic Surgery: Comprehensive Techniques and Pathologies Addressed by Full Endoscopy Beyond Lumbar Disc Herniation.J Clin Med. 2025 May 24;14(11):3685. doi: 10.3390/jcm14113685. J Clin Med. 2025. PMID: 40507448 Free PMC article. Review.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
