

Development of a nomogram for prediction of central lymph node metastasis of papillary thyroid microcarcinoma
- PMID: 38378515
- PMCID: PMC10877775
- DOI: 10.1186/s12885-024-12004-3
Development of a nomogram for prediction of central lymph node metastasis of papillary thyroid microcarcinoma
Abstract
Background: Papillary thyroid carcinoma (PTC) is the most frequent malignant tumor in thyroid carcinoma. The aim of this study was to explore the risk factors associated with central lymph node metastasis in papillary thyroid microcarcinoma (PTMC) and establish a nomogram model that can assess the probability of central lymph node metastasis (CLNM).
Methods: The clinicopathological data of 377 patients with cN0 PTMC were collected and analyzed from The Second Affiliated Hospital of Fujian Medical University from July 1st, 2019 to December 30th, 2021. All patients were examined by underwent ultrasound (US), found without metastasis to central lymph nodes, and diagnosed with PTMC through pathologic examination. All patients received thyroid lobectomy or total thyroidectomy with therapeutic or prophylactic central lymph node dissection (CLND). R software (Version 4.1.0) was employed to conduct a series of statistical analyses and establish the nomogram.
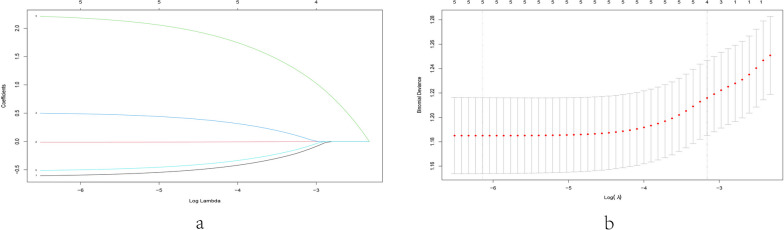
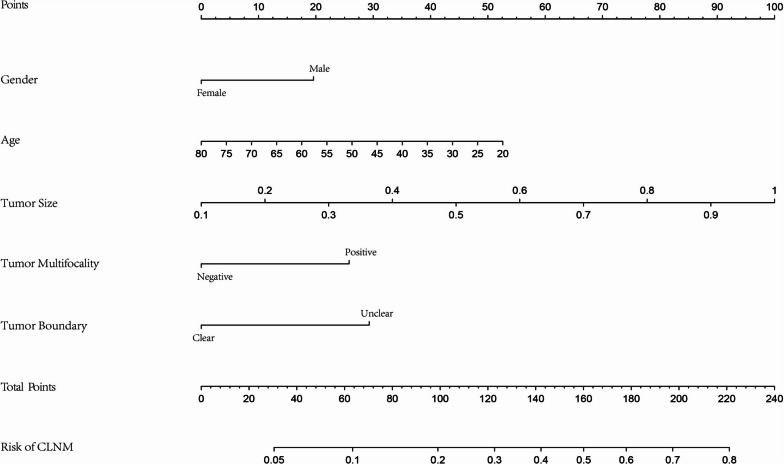
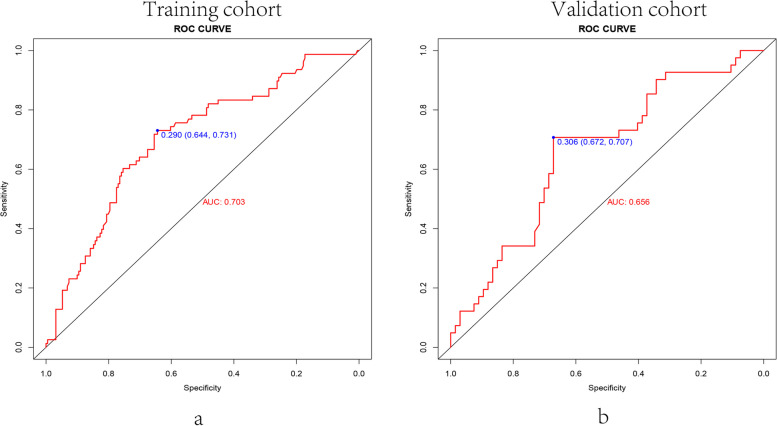
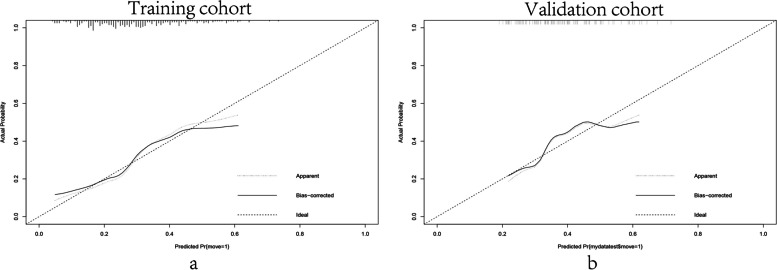
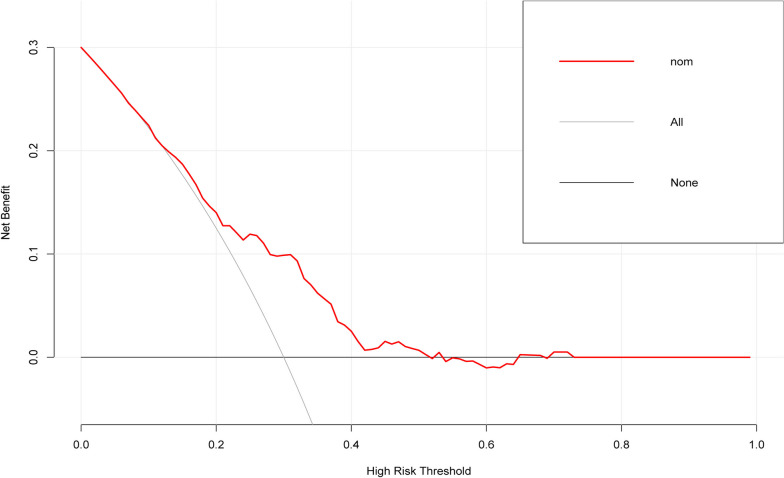
Results: A total of 119 patients with PTMC had central lymph node metastases (31.56%). After that, age (P < 0.05), gender (P < 0.05), tumor size (P < 0.05), tumor multifocality (P < 0.05), and ultrasound imaging-suggested tumor boundaries (P < 0.05) were identified as the risk factors associated with CLNM. Subsequently, multivariate logistic regression analysis indicated that the area under the receiver operating characteristic (ROC) curve (AUC) of the training cohort was 0.703 and that of the validation cohort was 0.656, demonstrating that the prediction ability of this model is relatively good compared to existing models. The calibration curves indicated a good fit for the nomogram model. Finally, the decision curve analysis (DCA) showed that a probability threshold of 0.15-0.50 could benefit patients clinically. The probability threshold used in DCA captures the relative value the patient places on receiving treatment for the disease, if present, compared to the value of avoiding treatment if the disease is not present.
Conclusion: CLNM is associated with many risk factors, including age, gender, tumor size, tumor multifocality, and ultrasound imaging-suggested tumor boundaries. The nomogram established in our study has moderate predictive ability for CLNM and can be applied to the clinical management of patients with PTMC. Our findings will provide a better preoperative assessment and treatment strategies for patients with PTMC whether to undergo central lymph node dissection.
Keywords: Central lymph node dissection (CLND); Decision curve analysis (DCA); Nomogram; Papillary thyroid microcarcinoma (PTMC).
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
The model for predicting the central lymph node metastasis in cN0 papillary thyroid microcarcinoma with Hashimoto's thyroiditis.Front Endocrinol (Lausanne). 2024 Apr 30;15:1330896. doi: 10.3389/fendo.2024.1330896. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 38745958 Free PMC article.
-
Nomogram for Preoperative Estimation of Cervical Lymph Node Metastasis Risk in Papillary Thyroid Microcarcinoma.Front Endocrinol (Lausanne). 2021 Mar 31;12:613974. doi: 10.3389/fendo.2021.613974. eCollection 2021. Front Endocrinol (Lausanne). 2021. PMID: 33868164 Free PMC article.
-
Identification of risk factors of central lymph node metastasis and evaluation of the effect of prophylactic central neck dissection on migration of staging and risk stratification in patients with clinically node-negative papillary thyroid microcarcinoma.Bull Cancer. 2017 Jun;104(6):516-523. doi: 10.1016/j.bulcan.2017.03.005. Epub 2017 May 2. Bull Cancer. 2017. PMID: 28476312
-
Risk Factors for Central Compartment Lymph Node Metastasis in Papillary Thyroid Microcarcinoma: A Meta-Analysis.World J Surg. 2015 Oct;39(10):2459-70. doi: 10.1007/s00268-015-3108-3. World J Surg. 2015. PMID: 26099728 Review.
-
Clinicopathologic predictors of central lymph node metastases in clinical node-negative papillary thyroid microcarcinoma: a systematic review and meta-analysis.World J Surg Oncol. 2022 Apr 1;20(1):106. doi: 10.1186/s12957-022-02573-7. World J Surg Oncol. 2022. PMID: 35365171 Free PMC article.
Cited by
-
Predictive nomogram for occult metastasis in central lymph nodes of papillary thyroid microcarcinoma based on clinical and ultrasound features.Gland Surg. 2025 Jul 31;14(7):1295-1305. doi: 10.21037/gs-2025-159. Epub 2025 Jul 28. Gland Surg. 2025. PMID: 40771386 Free PMC article.
-
Current evidence and strategies for preventing tumor recurrence following thermal ablation of papillary thyroid carcinoma.Cancer Imaging. 2025 Jul 9;25(1):88. doi: 10.1186/s40644-025-00908-7. Cancer Imaging. 2025. PMID: 40635097 Free PMC article. Review.
-
The impact of age at diagnosis on central lymph node metastasis in clinically low-risk papillary thyroid microcarcinoma patients.Thyroid Res. 2025 Mar 4;18(1):6. doi: 10.1186/s13044-025-00224-z. Thyroid Res. 2025. PMID: 40033421 Free PMC article.
-
Development of a clinical-molecular prediction model for central lymph node metastasis in cN0 stage papillary thyroid microcarcinoma: a retrospective study.BMC Cancer. 2025 Apr 14;25(1):693. doi: 10.1186/s12885-025-14112-0. BMC Cancer. 2025. PMID: 40229698 Free PMC article.
-
Development and validation of a multidimensional machine learning-based nomogram for predicting central lymph node metastasis in papillary thyroid microcarcinoma.Gland Surg. 2025 Mar 31;14(3):344-357. doi: 10.21037/gs-2024-508. Epub 2025 Mar 26. Gland Surg. 2025. PMID: 40256479 Free PMC article.
References
-
- Haugen B, Alexander E, Bible K, Doherty G, Mandel S, Nikiforov Y, Pacini F, Randolph G, Sawka A, Schlumberger M, et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26(1):1–133. doi: 10.1089/thy.2015.0020. - DOI - PMC - PubMed
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
