

Efficacy of Repeated Low-Level Red Light (RLRL) therapy on myopia outcomes in children: a systematic review and meta-analysis
- PMID: 38378527
- PMCID: PMC10877869
- DOI: 10.1186/s12886-024-03337-5
Efficacy of Repeated Low-Level Red Light (RLRL) therapy on myopia outcomes in children: a systematic review and meta-analysis
Abstract
Background: Myopia is the most prevalent form of refractive error that has a major negative impact on visual function and causes blurring of vision. We aimed to determine if Repeated Low-Level Red Light (RLRL) treatment is beneficial in treating childhood myopia in terms of axial length (AL), spherical equivalent refraction (SER), and sub foveal choroidal thickness (SFCT).
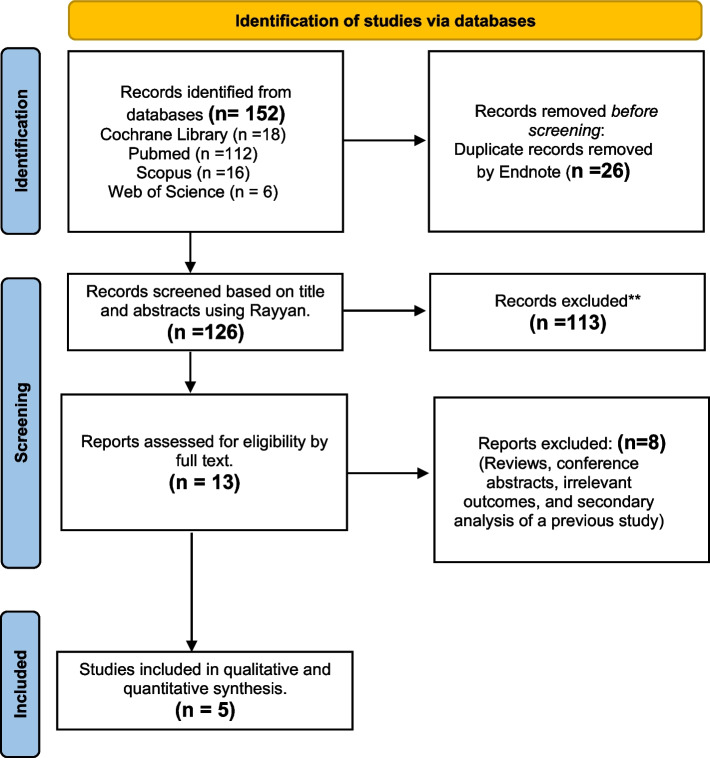
Methods: This systematic review was performed on RLRL for treatment of myopia in children compared to single vision spectacles (SVS). We employed the search strategy with key terms myopia and low-level light therapy then we searched PubMed, Scopus, Cochrane, and Web of Science databases. The mean differences (MD) were used to evaluate the treatment effects. Heterogeneity was quantified using I2 statistics and explored by sensitivity analysis.
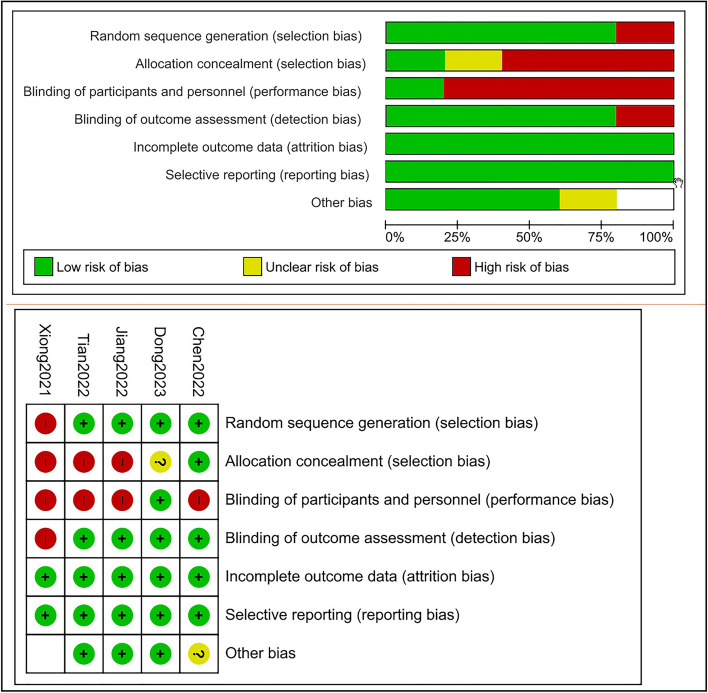
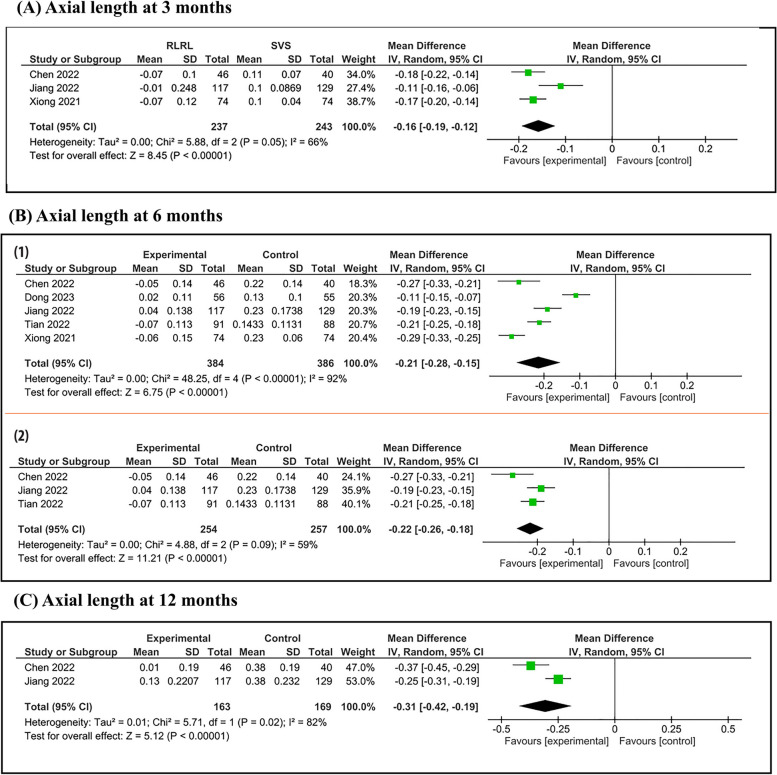
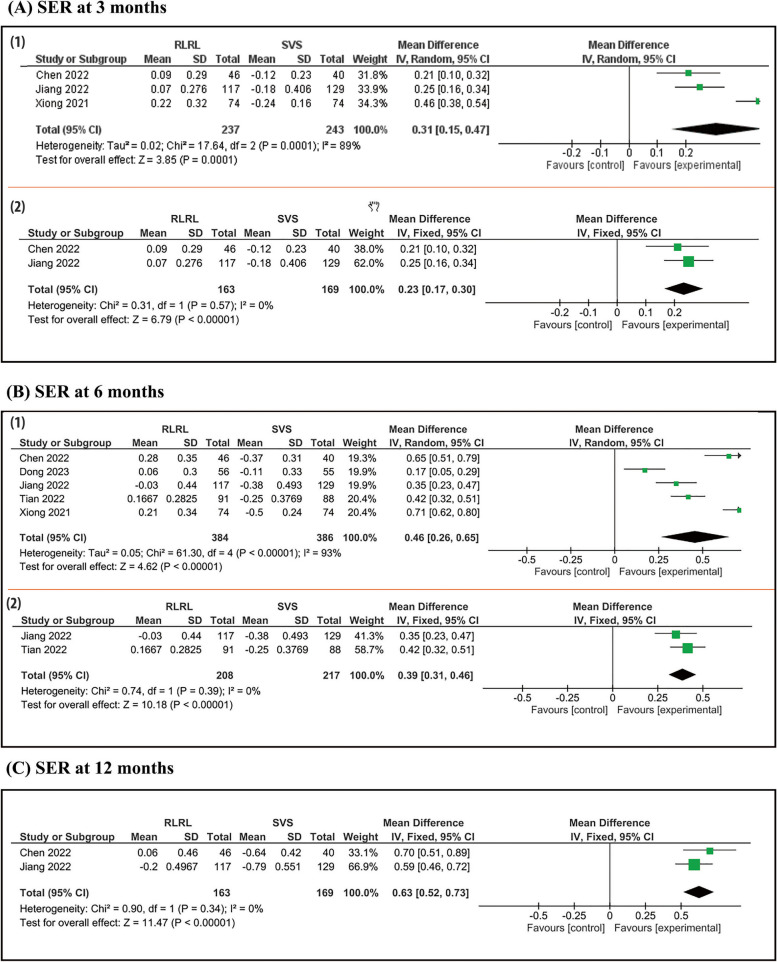
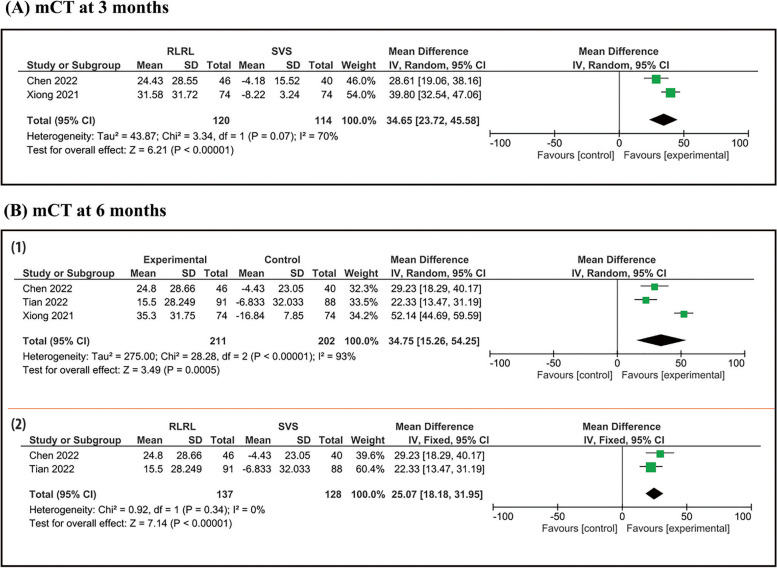
Results: Five randomized controlled trials (RCTs) were included in our meta-analysis with a total of 833 patients, 407 in treatment group and 426 in control group. At a 3 month follow up period, pooled studies show a statistical difference in AL between RLRL and SVS group (MD = -0.16; 95% CI [-0.19, -0.12], SER (MD = 0.33; 95% CI [0.27, 0.38]), and SFCT (MD = 43.65; 95% CI [23.72, 45.58]). At a 6 month follow up period, pooled studies show a statistical difference in AL between RLRL and SVS group (MD = -0.21; 95% CI [-0.28, -0.15]), SER (MD = 0.46; 95% CI [0.26, 0.65]), and SFCT (MD = 25.07; 95% CI [18.18, 31.95]). At a 12 month follow up period, pooled studies show a statistical difference in AL between RLRL and SVS group (MD = -0.31; 95% CI [-0.42, -0.19]) and SER (MD = 0.63; 95% CI [0.52, 0.73]).
Conclusion: This is the first systematic review and meta-analysis investigating only RCTs evidence supporting the efficacy of 650 nm RLRL for myopia control in the short term of 3, 6, and 12 months follow up. The present review revealed the clinical significance of RLRL as a new alternative treatment for myopia control with good user acceptability and no documented functional or structural damage. However, the effect of long-term RLRL treatment and the rebound effect after cessation require further investigations.
Keywords: Axial length (AL); Childhood myopia; Repeated Low-Level Red Light (RLRL); Spherical equivalent refraction (SER); Sub foveal choroidal thickness (SFCT).
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
