

Safety, feasibility, and impact on the gut microbiome of kefir administration in critically ill adults
- PMID: 38378568
- PMCID: PMC10880344
- DOI: 10.1186/s12916-024-03299-x
Safety, feasibility, and impact on the gut microbiome of kefir administration in critically ill adults
Abstract
Background: Dysbiosis of the gut microbiome is frequent in the intensive care unit (ICU), potentially leading to a heightened risk of nosocomial infections. Enhancing the gut microbiome has been proposed as a strategic approach to mitigate potential adverse outcomes. While prior research on select probiotic supplements has not successfully shown to improve gut microbial diversity, fermented foods offer a promising alternative. In this open-label phase I safety and feasibility study, we examined the safety and feasibility of kefir as an initial step towards utilizing fermented foods to mitigate gut dysbiosis in critically ill patients.
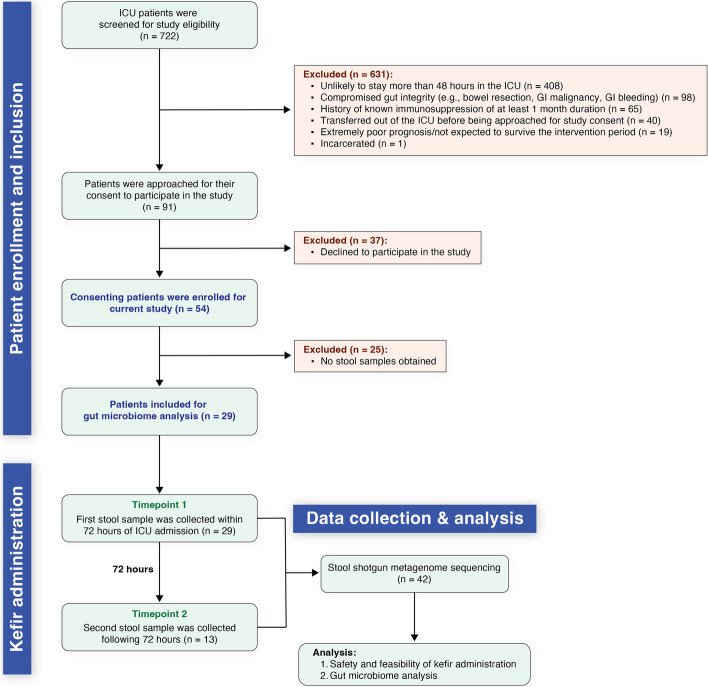
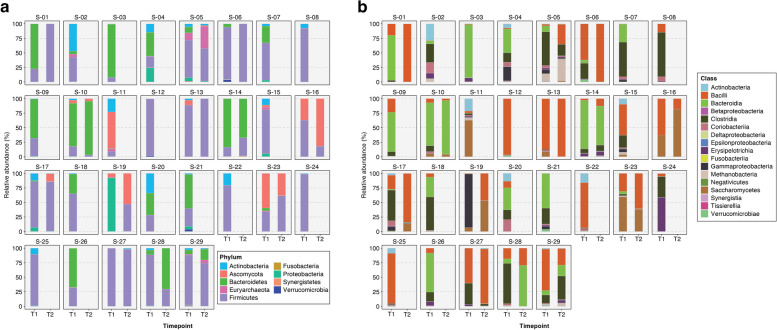
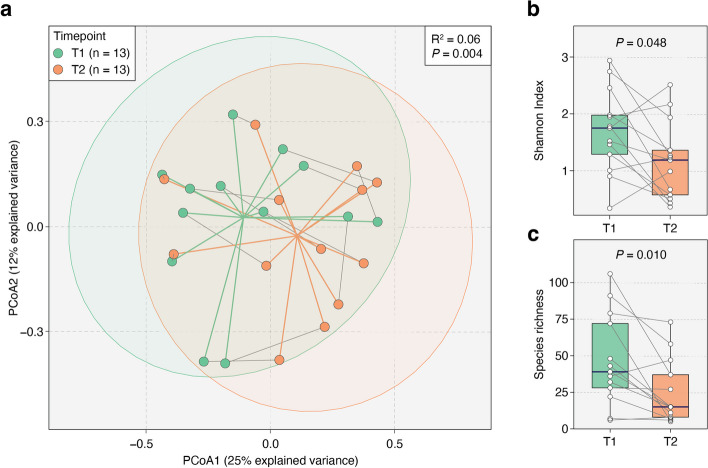
Methods: We administered kefir in escalating doses (60 mL, followed by 120 mL after 12 h, then 240 mL daily) to 54 critically ill patients with an intact gastrointestinal tract. To evaluate kefir's safety, we monitored for gastrointestinal symptoms. Feasibility was determined by whether patients received a minimum of 75% of their assigned kefir doses. To assess changes in the gut microbiome composition following kefir administration, we collected two stool samples from 13 patients: one within 72 h of admission to the ICU and another at least 72 h after the first stool sample.
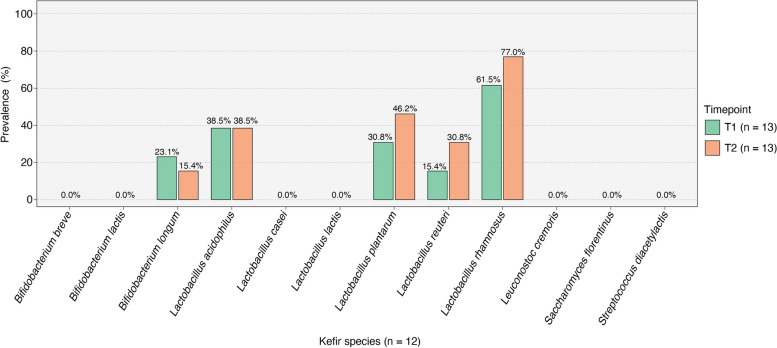
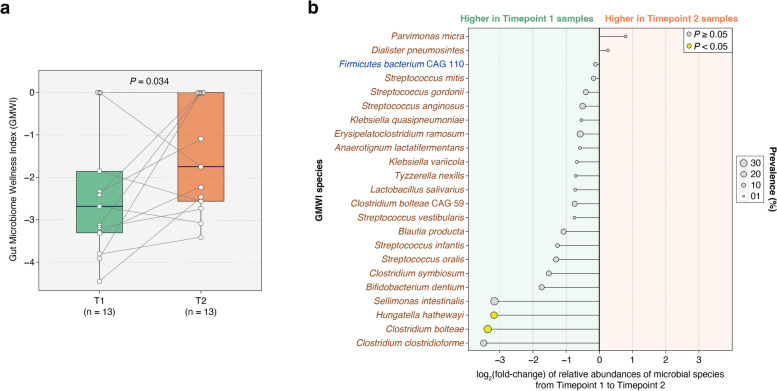
Results: After administering kefir, none of the 54 critically ill patients exhibited signs of kefir-related bacteremia. No side effects like bloating, vomiting, or aspiration were noted, except for diarrhea in two patients concurrently on laxatives. Out of the 393 kefir doses prescribed for all participants, 359 (91%) were successfully administered. We were able to collect an initial stool sample from 29 (54%) patients and a follow-up sample from 13 (24%) patients. Analysis of the 26 paired samples revealed no increase in gut microbial α-diversity between the two timepoints. However, there was a significant improvement in the Gut Microbiome Wellness Index (GMWI) by the second timepoint (P = 0.034, one-sided Wilcoxon signed-rank test); this finding supports our hypothesis that kefir administration can improve gut health in critically ill patients. Additionally, the known microbial species in kefir were found to exhibit varying levels of engraftment in patients' guts.
Conclusions: Providing kefir to critically ill individuals is safe and feasible. Our findings warrant a larger evaluation of kefir's safety, tolerability, and impact on gut microbiome dysbiosis in patients admitted to the ICU.
Trial registration: NCT05416814; trial registered on June 13, 2022.
Keywords: Critical illness; GMWI; Gut microbiome; ICU; Kefir; Probiotics.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Chernevskaya E, Beloborodova N, Klimenko N, Pautova A, Shilkin D, Gusarov V, Tyakht A. Serum and fecal profiles of aromatic microbial metabolites reflect gut microbiota disruption in critically ill patients: a prospective observational pilot study. Crit Care. 2020;24(1):312. doi: 10.1186/s13054-020-03031-0. - DOI - PMC - PubMed
-
- Lankelma JM, van Vught LA, Belzer C, Schultz MJ, van der Poll T, de Vos WM, Wiersinga WJ. Critically ill patients demonstrate large interpersonal variation in intestinal microbiota dysregulation: a pilot study. Intensive Care Med. 2017;43(1):59–68. doi: 10.1007/s00134-016-4613-z. - DOI - PMC - PubMed
-
- Belizário JE, Faintuch J. Microbiome and gut dysbiosis. In: Silvestre R, Torrado E, editors. Metabolic Interaction in Infection. Cham: Springer International Publishing; 2018. pp. 459–476.
-
- Zhang F, Wan Y, Zuo T, Yeoh YK, Liu Q, Zhang L, Zhan H, Lu W, Xu W, Lui GCY, et al. Prolonged impairment of short-chain fatty acid and L-isoleucine biosynthesis in gut microbiome in patients with COVID-19. Gastroenterology. 2022;162(2):548–561. doi: 10.1053/j.gastro.2021.10.013. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
