

Readmission after enhanced recovery video-assisted thoracoscopic surgery wedge resection
- PMID: 38379006
- PMCID: PMC10978727
- DOI: 10.1007/s00464-024-10700-6
Readmission after enhanced recovery video-assisted thoracoscopic surgery wedge resection
Abstract
Background: Despite the implementation of Enhanced Recovery After Surgery (ERAS) programs, surgical stress continues to influence postoperative rehabilitation, including the period after discharge. However, there is a lack of data available beyond the point of discharge following video-assisted thoracoscopic surgery (VATS) wedge resection. Therefore, the objective of this study is to investigate incidence and risk factors for readmissions after ERAS VATS wedge resection.
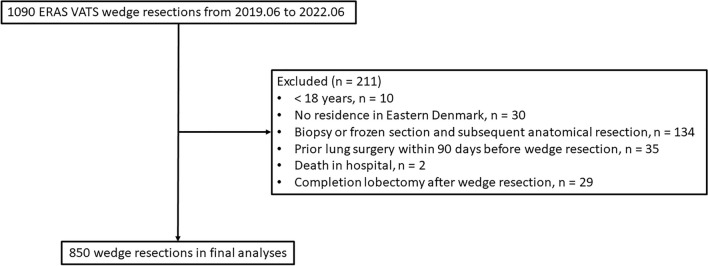
Methods: A retrospective analysis was performed on data from prospectively collected consecutive VATS wedge resections from June 2019 to June 2022. We evaluated main reasons related to wedge resection leading to 90-day readmission, early (occurring within 0-30 days postoperatively) and late readmission (occurring within 31-90 days postoperatively). To identify predictors for these readmissions, we utilized a logistic regression model for both univariable and multivariable analyses.
Results: A total of 850 patients (non-small cell lung cancer 21.5%, metastasis 44.7%, benign 31.9%, and other lung cancers 1.9%) were included for the final analysis. Median length of stay was 1 day (IQR 1-2). During the postoperative 90 days, 86 patients (10.1%) were readmitted mostly due to pneumonia and pneumothorax. Among the cohort, 66 patients (7.8%) had early readmissions primarily due to pneumothorax and pneumonia, while 27 patients (3.2%) experienced late readmissions mainly due to pneumonia, with 7 (0.8%) patients experiencing both early and late readmissions. Multivariable analysis demonstrated that male gender, pulmonary complications, and neurological complications were associated with readmission.
Conclusions: Readmission after VATS wedge resection remains significant despite an optimal ERAS program, with pneumonia and pneumothorax as the dominant reasons. Early readmission was primarily associated with pneumothorax and pneumonia, while late readmission correlated mainly with pneumonia.
Keywords: Enhanced recovery after surgery; Postoperative adverse events; Pulmonary wedge resection; Readmission; Video-assisted thoracoscopic surgery.
© 2024. The Author(s).
Conflict of interest statement
René Horsleben Petersen reports speaker fee from Medtronic, Medela, AstraZeneca and AMBU, advisory board member for AstraZeneca, MSD, BMS and Roche. Lin Huang and Henrik Kehlet have no conflict of interest to report.
Figures


Similar articles
-
Early and late readmissions after enhanced recovery thoracoscopic lobectomy.Eur J Cardiothorac Surg. 2022 Aug 3;62(3):ezac385. doi: 10.1093/ejcts/ezac385. Eur J Cardiothorac Surg. 2022. PMID: 35880263
-
National Assessment of Early Discharge After Video-Assisted Thoracoscopic Surgery for Lung Resection.J Surg Res. 2022 Aug;276:242-250. doi: 10.1016/j.jss.2022.02.025. Epub 2022 Apr 5. J Surg Res. 2022. PMID: 35395564
-
Incidence and risk factors for 90-day hospital readmission following video-assisted thoracoscopic anatomical lung resection†.Eur J Cardiothorac Surg. 2019 Apr 1;55(4):666-672. doi: 10.1093/ejcts/ezy345. Eur J Cardiothorac Surg. 2019. PMID: 30364954
-
Risk of Pneumothorax Requiring Pleural Drainage after Drainless VATS Pulmonary Wedge Resection: A Systematic Review and Meta-Analysis.Innovations (Phila). 2022 Jan-Feb;17(1):14-24. doi: 10.1177/15569845221074431. Innovations (Phila). 2022. PMID: 35225064
-
In patients with resectable non-small-cell lung cancer, is video-assisted thoracoscopic segmentectomy a suitable alternative to thoracotomy and segmentectomy in terms of morbidity and equivalence of resection?Interact Cardiovasc Thorac Surg. 2014 Jul;19(1):107-10. doi: 10.1093/icvts/ivu080. Epub 2014 Apr 10. Interact Cardiovasc Thorac Surg. 2014. PMID: 24722517 Review.
Cited by
-
A Smartphone App for the Management of Postoperative Home Recovery After Thoracic Surgery Procedures: A Pilot Study Using the Care4Today™ App.J Clin Med. 2024 Dec 23;13(24):7843. doi: 10.3390/jcm13247843. J Clin Med. 2024. PMID: 39768766 Free PMC article.
-
Risk factors for postoperative pulmonary complications in elderly patients undergoing video-assisted thoracoscopic surgery lobectomy under general anesthesia: a retrospective study.BMC Surg. 2024 May 14;24(1):153. doi: 10.1186/s12893-024-02444-w. BMC Surg. 2024. PMID: 38745149 Free PMC article.
References
-
- Batchelor TJP, Rasburn NJ, Abdelnour-Berchtold E, Brunelli A, Cerfolio RJ, Gonzalez M, Ljungqvist O, Petersen RH, Popescu WM, Slinger PD, Naidu B. Guidelines for enhanced recovery after lung surgery: recommendations of the enhanced recovery after surgery (ERAS(R)) Society and the European Society of Thoracic Surgeons (ESTS) Eur J Cardiothorac Surg. 2019;55:91–115. doi: 10.1093/ejcts/ezy301. - DOI - PubMed
-
- Kehlet H. Enhanced postoperative recovery: good from afar, but far from good? Anaesthesia. 2020;75(Suppl 1):e54–e61. - PubMed
-
- Seder CW, Salati M, Kozower BD, Wright CD, Falcoz PE, Brunelli A, Fernandez FG. Variation in pulmonary resection practices between the society of thoracic surgeons and the European society of thoracic surgeons general thoracic surgery databases. Ann Thorac Surg. 2016;101:2077–2084. doi: 10.1016/j.athoracsur.2015.12.073. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
