

Concomitant atrial fibrillation ablation in minimally invasive cardiac surgery
- PMID: 38380139
- PMCID: PMC10875199
- DOI: 10.21037/acs-2023-afm-21
Concomitant atrial fibrillation ablation in minimally invasive cardiac surgery
Abstract
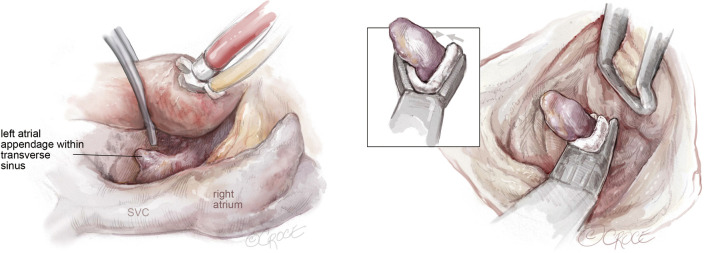
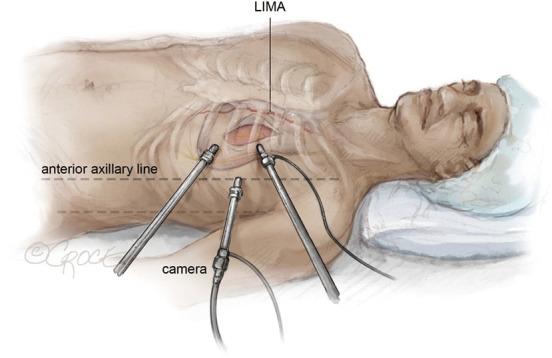
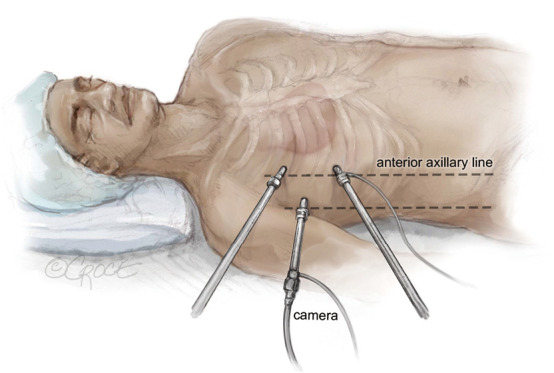
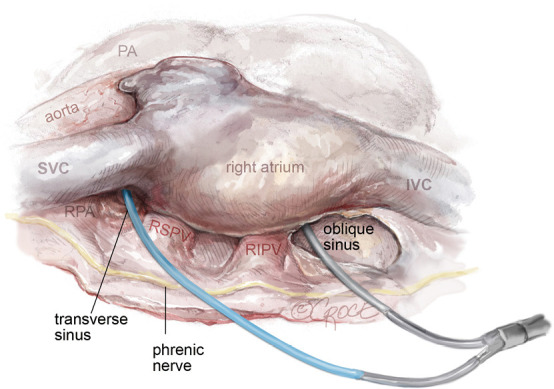
Concomitant atrial fibrillation (AF) ablation in cardiac surgery effectively restores sinus rhythm and may reduce morbidity and mortality. Cardiac surgery has witnessed the transition from the historical Cox Maze procedure to more modern and less invasive approaches for concomitant AF treatment. As minimally invasive cardiac surgery gains traction, ablation methods and careful patient selection become crucial to optimize results. Emerging techniques, including bipolar epicardial radiofrequency and endo/epicardial cryoablation, are central to these advances, targeting specific arrhythmogenic areas within the atria. While pulmonary vein isolation (PVI) is essential, it may be insufficient for patients with persistent or longstanding persistent AF. In such cases, left atrial posterior wall isolation has proven beneficial. Furthermore, recent studies emphasize the significance of left atrial appendage occlusion in concurrent AF treatments, highlighting its role in stroke risk reduction. Notably, the left atrium remains the focal point for concomitant AF surgery over the right, primarily due to concerns like high pacemaker implantation rates and complexities of right atrial ablation sets. Although guidelines support its widespread use, concomitant AF ablation outcomes vary based on patient selection, surgeon's expertise, and clinical context and thus the Heart Team's input is crucial for individualized decisions. In the upcoming sections, we present our patient selection and a visual guide to our techniques for concomitant AF surgery in minimally invasive mitral valve, coronary artery bypass and aortic valve surgery.
Keywords: Atrial fibrillation (AF); cardiac surgery; minimally invasive ablation.
2024 Annals of Cardiothoracic Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: F.A., T.J.B. and N.V. are proctor for Medtronic. The authors have no other conflicts of interest to declare.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources