

Amplitude spectral area of ventricular fibrillation can discriminate survival of patients with out-of-hospital cardiac arrest
- PMID: 38380178
- PMCID: PMC10876863
- DOI: 10.3389/fcvm.2024.1336291
Amplitude spectral area of ventricular fibrillation can discriminate survival of patients with out-of-hospital cardiac arrest
Abstract
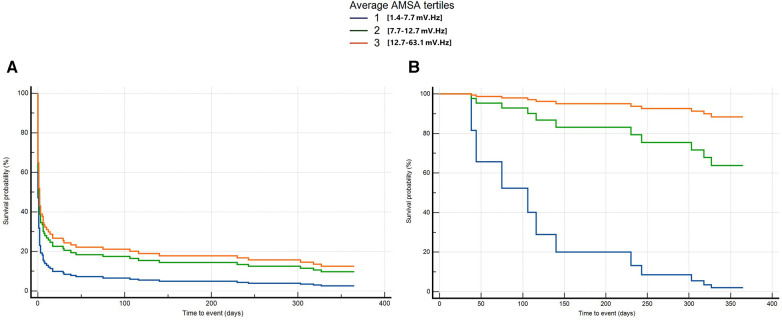
Background: Evidence of the association between AMplitude Spectral Area (AMSA) of ventricular fibrillation and outcome after out-of-hospital cardiac arrest (OHCA) is limited to short-term follow-up. In this study, we assess whether AMSA can stratify the risk of death or poor neurological outcome at 30 days and 1 year after OHCA in patients with an initial shockable rhythm or with an initial non-shockable rhythm converted to a shockable one.
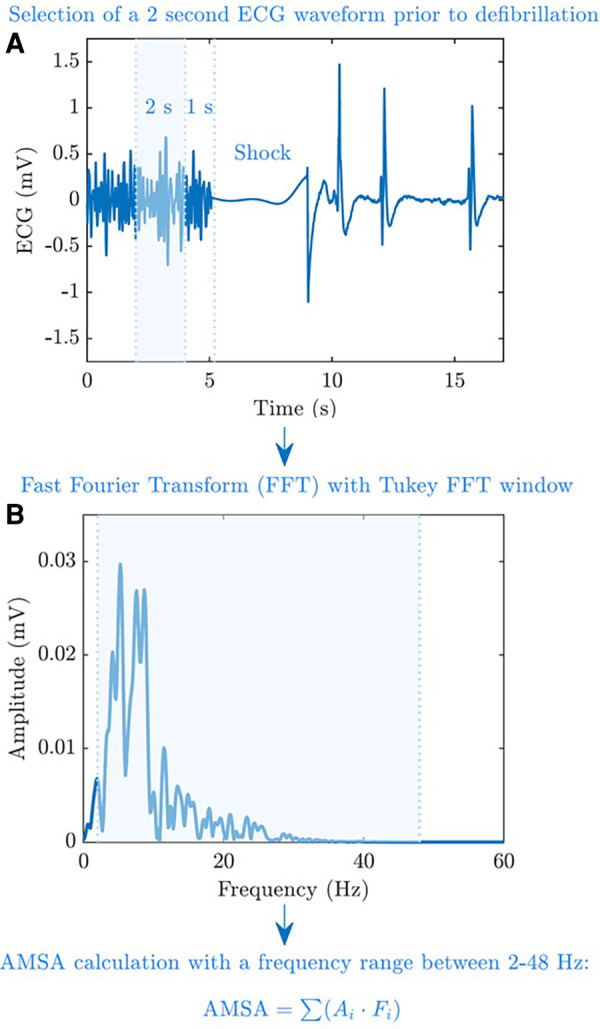
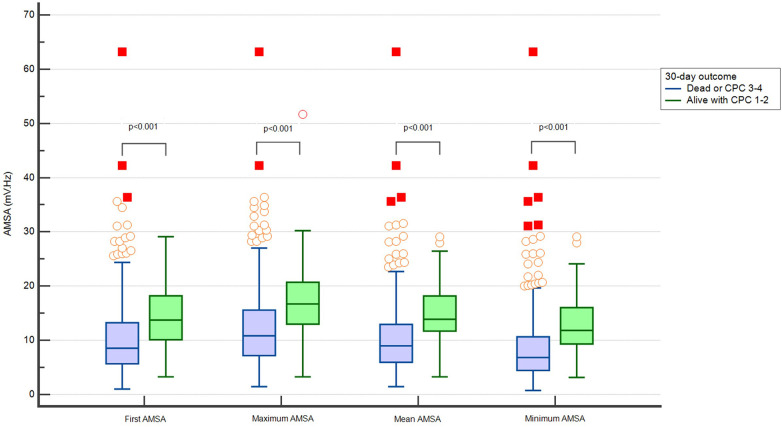
Methods: This is a multicentre retrospective study of prospectively collected data in two European Utstein-based OHCA registries. We included all cases of OHCAs with at least one manual defibrillation. AMSA values were calculated after data extraction from the monitors/defibrillators used in the field by using a 2-s pre-shock electrocardiogram interval. The first detected AMSA value, the maximum value, the average value, and the minimum value were computed, and their outcome prediction accuracy was compared. Multivariable Cox regression models were run for both 30-day and 1-year deaths or poor neurological outcomes. Neurological cerebral performance category 1-2 was considered a good neurological outcome.
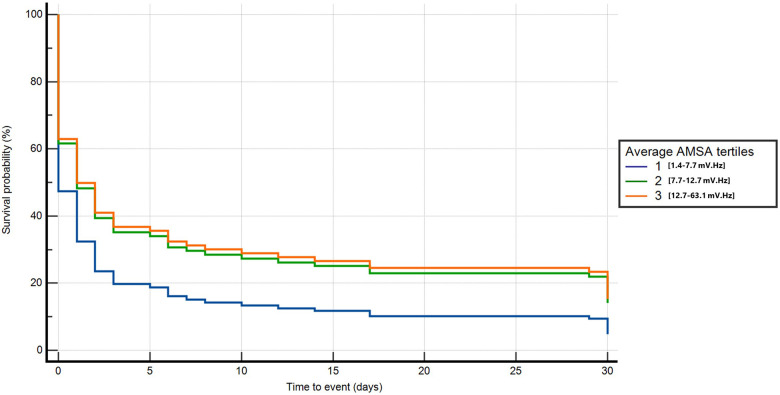
Results: Out of the 578 patients included, 494 (85%) died and 10 (2%) had a poor neurological outcome at 30 days. All the AMSA values considered (first value, maximum, average, and minimum) were significantly higher in survivors with good neurological outcome at 30 days. The average AMSA showed the highest area under the receiver operating characteristic curve (0.778, 95% CI: 0.7-0.8, p < 0.001). After correction for confounders, the highest tertiles of average AMSA (T3 and T2) were significantly associated with a lower risk of death or poor neurological outcome compared with T1 both at 30 days (T2: HR 0.6, 95% CI: 0.4-0.9, p = 0.01; T3: HR 0.6, 95% CI: 0.4-0.9, p = 0.02) and at 1 year (T2: HR 0.6, 95% CI: 0.4-0.9, p = 0.01; T3: HR 0.6, 95% CI: 0.4-0.9, p = 0.01). Among survivors at 30 days, a higher AMSA was associated with a lower risk of mortality or poor neurological outcome at 1 year (T3: HR 0.03, 95% CI: 0-0.3, p = 0.02).
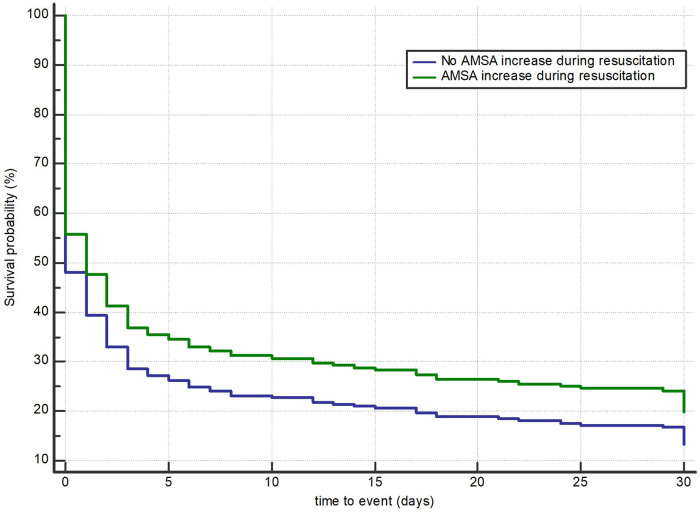
Discussion: Lower AMSA values were significantly and independently associated with the risk of death or poor neurological outcome at 30 days and at 1 year in OHCA patients with either an initial shockable rhythm or a conversion rhythm from non-shockable to shockable. The average AMSA value had the strongest association with prognosis.
Keywords: AMSA; OHCA; cardiac arrest; defibrillation; survival; ventricular fibrillation.
© 2024 Gentile, Wik, Isasi, Baldi, Aramendi, Steen-Hansen, Fasolino, Compagnoni, Contri, Palo, Primi, Bendotti, Currao, Quilico, Vicini Scajola, Lopiano and Savastano.
Conflict of interest statement
LW was PI in the Zoll Medical–funded CIRC study and holds several patents via Oslo University Hospital (Inven2). He is a member of the medical advisory board of Stryker/Physio-Control. SS, EB, and EC are part of ERC Research NET. SS and EB are part of ESCAPE-NET. FRG, EB, EA, AF, AC, and SS are part of the COST action PARQ. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The reviewer TS declared a past co-authorship with the authors EB, RP, and SS to the handling editor. The authors declared that they were editorial board members of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures
References
-
- Nishiyama C, Kiguchi T, Okubo M, Alihodžić H, Al-Araji R, Baldi E, et al. Three-year trends in out-of-hospital cardiac arrest across the world: second report from the international liaison committee on resuscitation (ILCOR). Resuscitation. (2023) 186:109757. 10.1016/j.resuscitation.2023.109757 - DOI - PubMed
LinkOut - more resources
Full Text Sources