

Direct anterior approach with conventional instruments versus robotic posterolateral approach in elective total hip replacement for primary osteoarthritis: a case-control study
- PMID: 38381320
- PMCID: PMC10881946
- DOI: 10.1186/s10195-024-00753-7
Direct anterior approach with conventional instruments versus robotic posterolateral approach in elective total hip replacement for primary osteoarthritis: a case-control study
Abstract
Background: The purpose of this study is to compare peri-operative and short-term outcomes in patients who underwent elective total hip replacement (THA) for primary osteoarthritis (OA) with direct anterior approach (DAA) versus a pair-matched cohort of patients who underwent robotic-assisted THA with posterolateral approach.
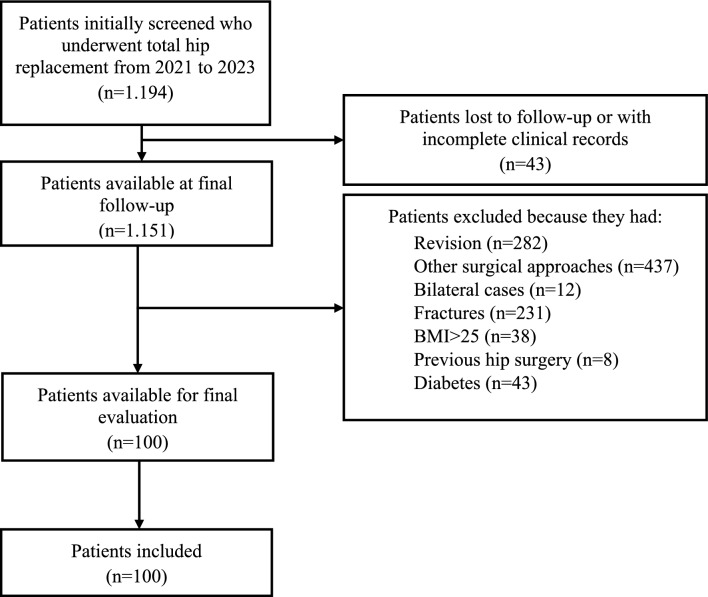
Materials and methods: Data from consecutive patients who underwent elective hip replacement from 2021 to 2023 for primary OA were retrospectively retrieved and divided into two groups: the DAA group, who underwent THA with the DAA approach using conventional instruments, and the robotic posterolateral (R-PL group), who underwent robot arm-assisted THA with the posterolateral approach. Comparative assessed outcomes were: operative time, radiographical implant positioning, intake of rescue analgesics, blood loss, transfusion rate, leg length discrepancy and functional outcomes (Harris hip score and forgotten joint score).
Results: A total of 100 pair-matched patients were retrieved with a mean age of 66.7 ± 10.7 (range: 32-85) years and a mean follow-up of 12.8 ± 3.6 (range: 7-24) months. No differences in patients' characteristics were detected. Patients in the R-PL group required less rescue tramadol (p > 0.001), ketorolac (p = 0.028) and acetaminophen (p < 0.001). There was no significant difference in the operative time between (MD = 5.0 min; p = 0.071). Patients in the DAA group had significantly lower Hb levels at day 1 (p = 0.002) without significant differences in transfusion rate (p = 0.283). Patients in the R-PL group had shorter length of stay (LOS) with a mean difference of 1.8 days [p < 0.001; 95% confidence interval (CI) 1.4-2.3]. No difference in clinical outcomes was found [leg length discrepancy (LLD), p = 0.572; HHS, p = 0.558; forgotten joint score (FJS), p = 0.629]. No radiographical differences were measured in cup inclination (MD = 2.0°, p = 0.069), malpositioning [odd ratio (OR) = 0.2; p = 0.141], stem alignment (OR = 0.3; p = 0.485) and stem sizing (OR = 1.5; p = 1.000). There was no difference in complication rate except for lateral femoral cutaneous nerve damage, which was higher in DAA group (p < 0.001).
Conclusions: R-PL and DAA THA had comparable short-term clinical and radiological outcomes along with similar complication rates. The R-PL group showed significantly lower Hb drop, rescue analgesic consumption and shorter LOS. This is a preliminary study and no strong recommendation can be provided. Further prospective randomized trials are requested to further investigate the cost-effectiveness of robotic surgery in THA.
Level of evidence: Level IV, case-control study.
Keywords: Anterior approach; MAKO; Osteoarthritis; Posterolateral total hip replacement; Robotic arthroplasty.
© 2024. The Author(s).
Conflict of interest statement
Other authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
Figures
References
-
- Geilen JEJW, Hermans SMM, Droeghaag R, Schotanus MGM, van Haaren EH, van Hemert WLW. A systematic review comparing the cost-effectiveness of the direct anterior, posterior, and straight lateral approach in total hip arthroplasty. EFORT Open Rev. 2023;8:443–450. doi: 10.1530/EOR-22-0108. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
