

Re-engagement and retention in HIV care after preventive default tracking in a cohort of HIV-infected patients in rural Malawi: A mixed-methods study
- PMID: 38381760
- PMCID: PMC10880992
- DOI: 10.1371/journal.pgph.0002437
Re-engagement and retention in HIV care after preventive default tracking in a cohort of HIV-infected patients in rural Malawi: A mixed-methods study
Abstract
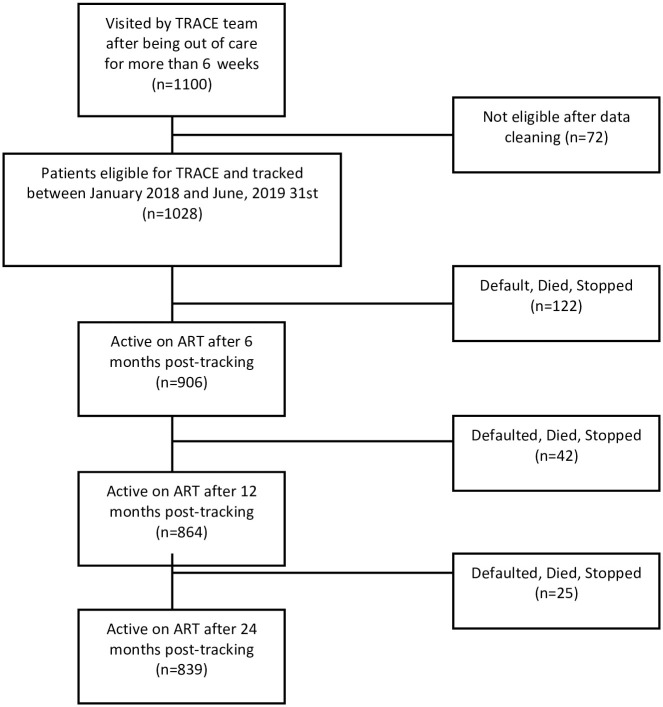
Loss-to-follow-up (LTFU) in the era of test-and-treat remains a universal challenge, especially in rural areas. To mitigate LTFU, the HIV program in Neno District, Malawi, utilizes a preventive default tracking strategy named Tracking for Retention and Client Enrollment (TRACE). We utilized a mixed-methods descriptive study of the TRACE program on patient's re-engagement and retention in care (RiC). In the quantitative arm, we utilized secondary data of HIV-infected patients in the TRACE program from January 2018 to June 2019 and analyzed patients' outcomes at 6-, 12-, and 24-months post-tracking. In the qualitative arm, we analyzed primary data from 25 semi-structured interviews. For the study period, 1028 patients were eligible with median age was 30 years, and 52% were women. We found that after tracking, 982 (96%) of patients with a 6-week missed appointment returned to care. After returning to care, 906 (88%), 864 (84%), and 839 (82%) were retained in care respectively at 6-,12-, and 24-months. In the multivariate analysis, which included all the covariates from the univariate analysis (including gender, BMI, age, and the timing of ART initiation), the results showed that RiC at 6 months was linked to WHO stage IV at the start of treatment (with an adjusted odds ratio (aOR) of 0.18; 95% confidence interval (CI) of 0.06-0.54) and commencing ART after the test-and-treat recommendation (aOR of 0.08; 95% CI: 0.06-0.18). RiC after 12 months was associated with age between 15 and 29 years (aOR = 0.18; 95%CI: 0.03-0.88), WHO stage IV (aOR = 0.12; 95%CI: 0.04-0.16) and initiating ART after test-and-treat recommendations (aOR = 0.08; 95%CI: 0.04-0.16). RiC at 24 months post-tracking was associated with being male (aOR = 0.61; 95%CI: 0.40-0.92) and initiating ART after test-and-treat recommendations (aOR = 0.16; 95%CI:0.10-0.25). The qualitative analysis revealed that clarity of the visit's purpose, TRACE's caring approach changed patient's mindset, enhanced sense of responsibility and motivated patients to resume care. We recommend integrating tracking programs in HIV care as it led to increase patient follow up and patient behavior change.
Copyright: © 2024 Suffrin et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
I have read the journal’s policy and the following authors of this manuscript have the following competing interests: Anat Rosenthal is an editorial board member of PLOS Global Public Health. The other Authors have no other conflicts of interests.
Figures


References
-
- Global Statistics | HIV.gov. [cited 22 Nov 2021]. https://www.hiv.gov/hiv-basics/overview/data-and-trends/global-statistics
-
- ANTIRETROVIRAL TOS. Guideline on when to start antiretroviral therapy and on pre-exposure prophylaxis for HIV. 2015. - PubMed
-
- Global HIV Programme. In: world Health Organization [Internet]. 2023 [cited 10 Nov 2023]. https://www.who.int/data/gho/data/themes/hiv-aids/data-on-the-hiv-aids-r...
-
- Gonzalo T, Goñi M, Muñoz-Fernández MA. Socio-Economic Impact of Antiretroviral Treatment in HIV patients. An Economic Review of Cost Savings after Introduction of HAART. AIDS Rev. 2008;11: 79–90. - PubMed
LinkOut - more resources
Full Text Sources