

Effect of Aspirin Versus Low-Molecular-Weight Heparin Thromboprophylaxis on Medication Satisfaction and Out-of-Pocket Costs: A Secondary Analysis of a Randomized Clinical Trial
- PMID: 38381842
- PMCID: PMC10980176
- DOI: 10.2106/JBJS.23.00824
Effect of Aspirin Versus Low-Molecular-Weight Heparin Thromboprophylaxis on Medication Satisfaction and Out-of-Pocket Costs: A Secondary Analysis of a Randomized Clinical Trial
Abstract
Background: Current guidelines recommend low-molecular-weight heparin for thromboprophylaxis after orthopaedic trauma. However, recent evidence suggests that aspirin is similar in efficacy and safety. To understand patients' experiences with these medications, we compared patients' satisfaction and out-of-pocket costs after thromboprophylaxis with aspirin versus low-molecular-weight heparin.
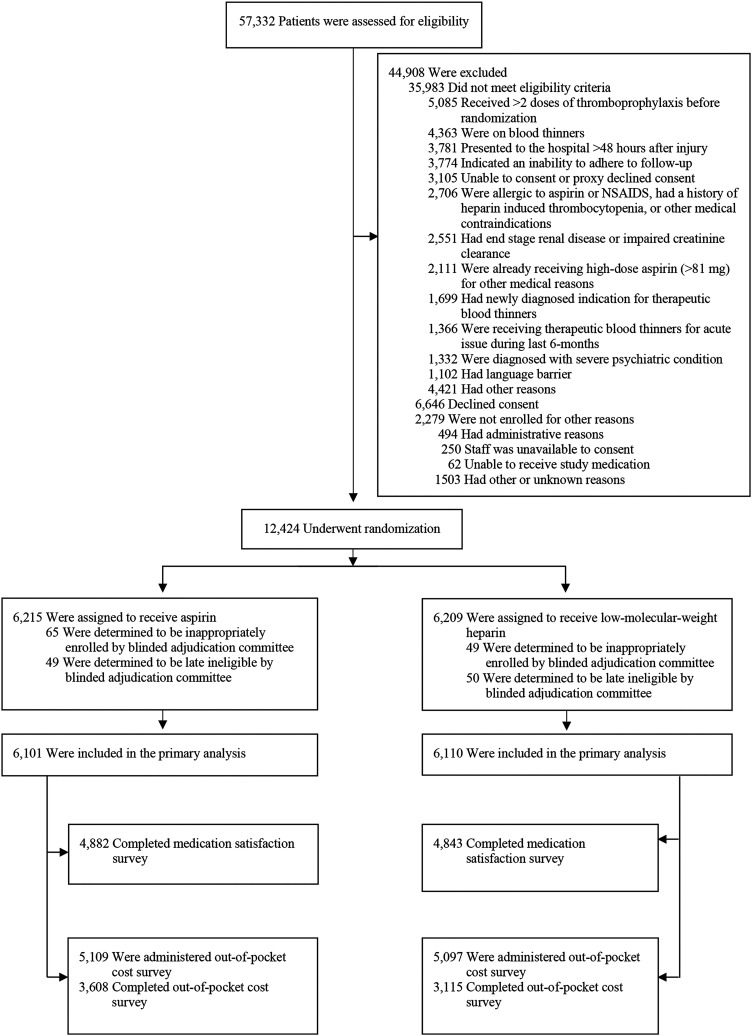
Methods: This study was a secondary analysis of the PREVENTion of CLots in Orthopaedic Trauma (PREVENT CLOT) trial, conducted at 21 trauma centers in the U.S. and Canada. We included adult patients with an operatively treated extremity fracture or a pelvic or acetabular fracture. Patients were randomly assigned to receive 30 mg of low-molecular-weight heparin (enoxaparin) twice daily or 81 mg of aspirin twice daily for thromboprophylaxis. The duration of the thromboprophylaxis, including post-discharge prescription, was based on hospital protocols. The study outcomes included patient satisfaction with and out-of-pocket costs for their thromboprophylactic medication measured on ordinal scales.
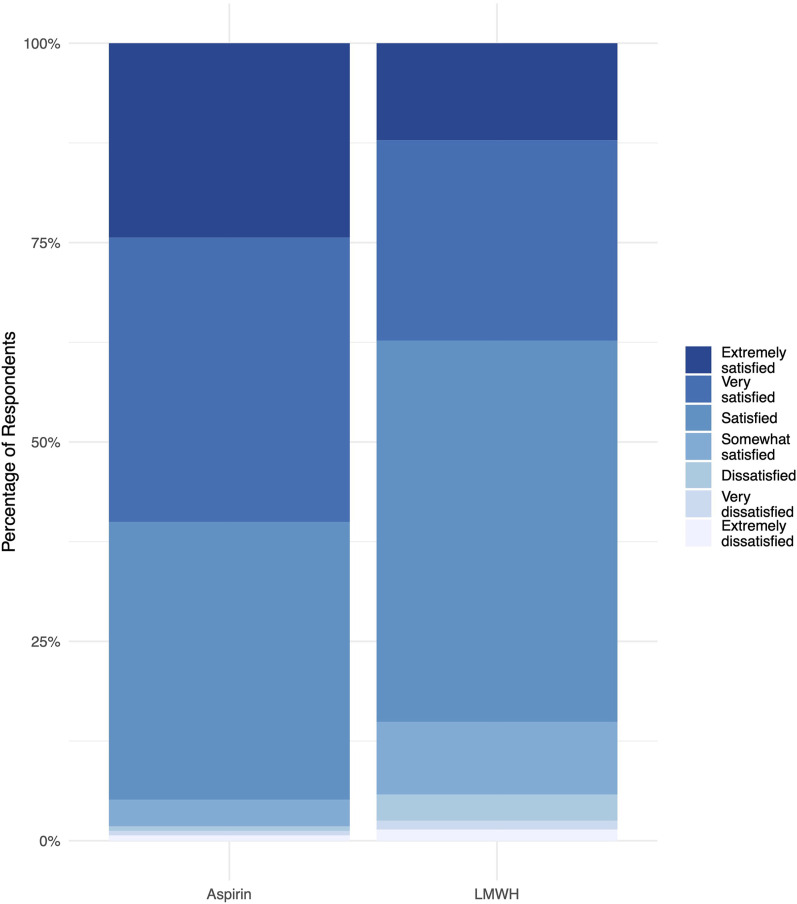
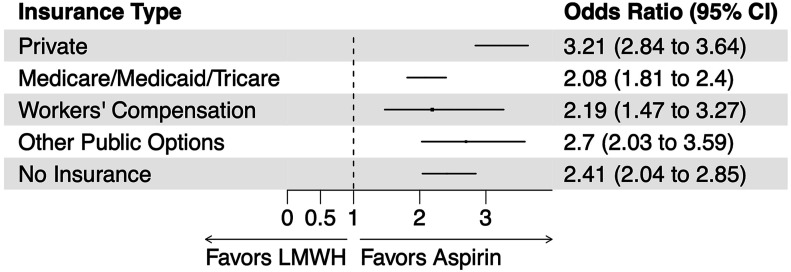
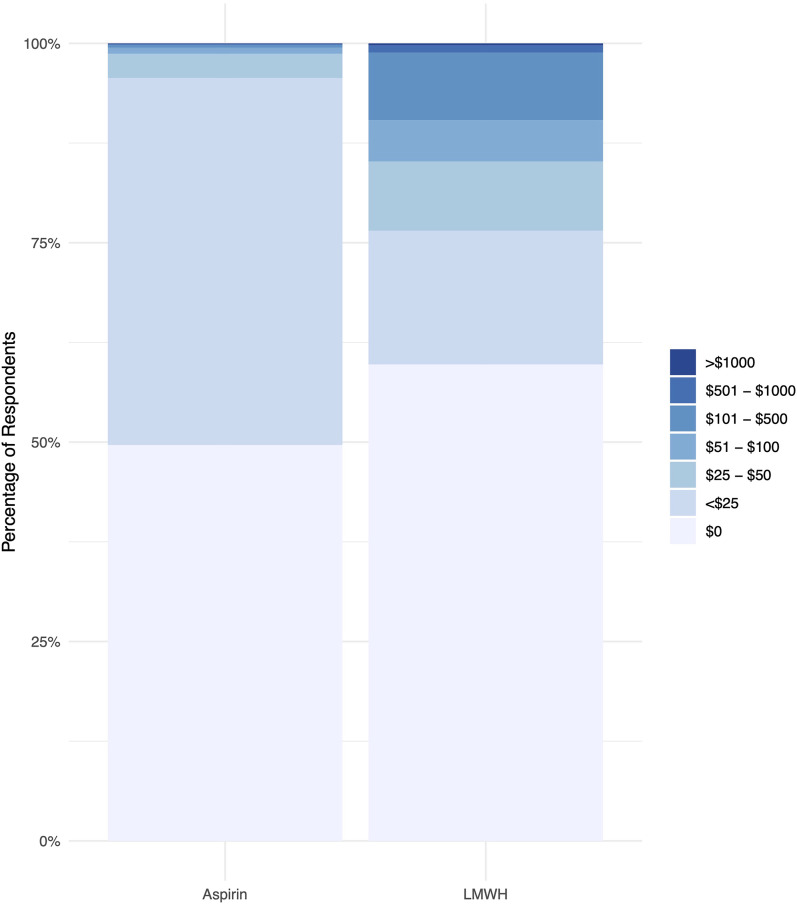
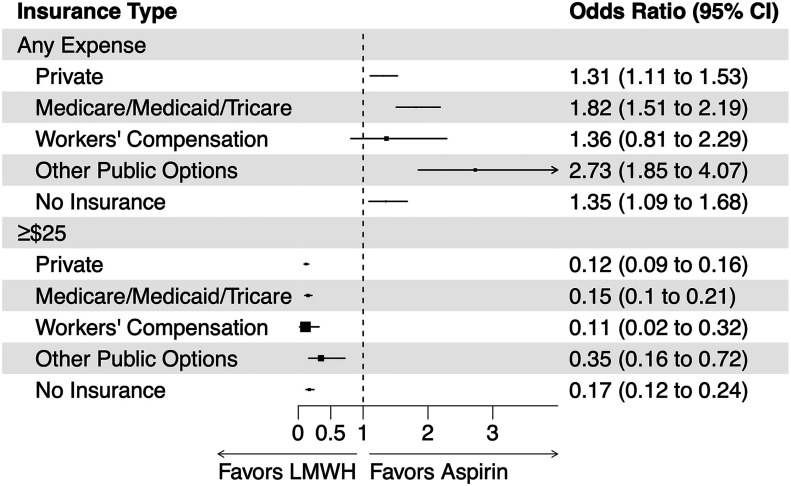
Results: The trial enrolled 12,211 patients (mean age and standard deviation [SD], 45 ± 18 years; 62% male), 9725 of whom completed the question regarding their satisfaction with the medication and 6723 of whom reported their out-of-pocket costs. The odds of greater satisfaction were 2.6 times higher for patients assigned to aspirin than those assigned to low-molecular-weight heparin (odds ratio [OR]: 2.59; 95% confidence interval [CI]: 2.39 to 2.80; p < 0.001). Overall, the odds of incurring any out-of-pocket costs for thromboprophylaxis medication were 51% higher for patients assigned to aspirin compared with low-molecular-weight heparin (OR: 1.51; 95% CI: 1.37 to 1.66; p < 0.001). However, patients assigned to aspirin had substantially lower odds of out-of-pocket costs of at least $25 (OR: 0.15; 95% CI: 0.12 to 0.18; p < 0.001).
Conclusions: Use of aspirin substantially improved patients' satisfaction with their medication after orthopaedic trauma. While aspirin use increased the odds of incurring any out-of-pocket costs, it protected against costs of ≥$25, potentially improving health equity for thromboprophylaxis.
Level of evidence: Therapeutic Level II . See Instructions for Authors for a complete description of levels of evidence.
Copyright © 2024 The Authors. Published by The Journal of Bone and Joint Surgery, Incorporated. All rights reserved.
Conflict of interest statement
Disclosure: This study was funded by the Patient-Centered Outcomes Research Institute (PCS-1511-32745 and DI-2022C3-29701). The Disclosure of Potential Conflicts of Interest forms are provided with the online version of the article ( http://links.lww.com/JBJS/H893 ).
Figures
References
-
- Barrera LM, Perel P, Ker K, Cirocchi R, Farinella E, Morales Uribe CH. Thromboprophylaxis for trauma patients. Cochrane Database Syst Rev. 2013 Mar 28;(3):CD008303. - PubMed
-
- Geerts WH, Code KI, Jay RM, Chen E, Szalai JP. A prospective study of venous thromboembolism after major trauma. N Engl J Med. 1994 Dec 15;331(24):1601-6. - PubMed
-
- Haut ER, Chang DC, Pierce CA, Colantuoni E, Efron DT, Haider AH, Cornwell EE, 3rd, Pronovost PJ. Predictors of posttraumatic deep vein thrombosis (DVT): hospital practice versus patient factors-an analysis of the National Trauma Data Bank (NTDB). J Trauma. 2009 Apr;66(4):994-9, discussion 999-1001. - PubMed
-
- Falck-Ytter Y, Francis CW, Johanson NA, Curley C, Dahl OE, Schulman S, Ortel TL, Pauker SG, Colwell CW, Jr. Prevention of VTE in orthopedic surgery patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2)(Suppl):e278S-325S. - PMC - PubMed
