

Parietal endometriosis: An uncommon cause of c-section scar pain - A case report
- PMID: 38382146
- PMCID: PMC10943926
- DOI: 10.1016/j.ijscr.2024.109410
Parietal endometriosis: An uncommon cause of c-section scar pain - A case report
Abstract
Introduction: Parietal endometriosis is the most common form of extra-pelvic endometriosis. It develops on the surgical scar of c-section or hysterectomy. It is one of the causes of scar pain.
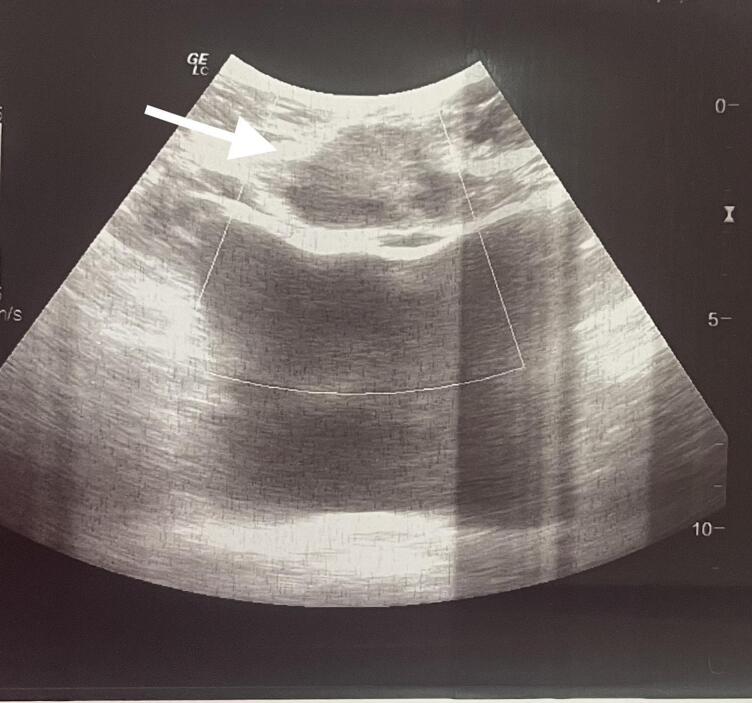
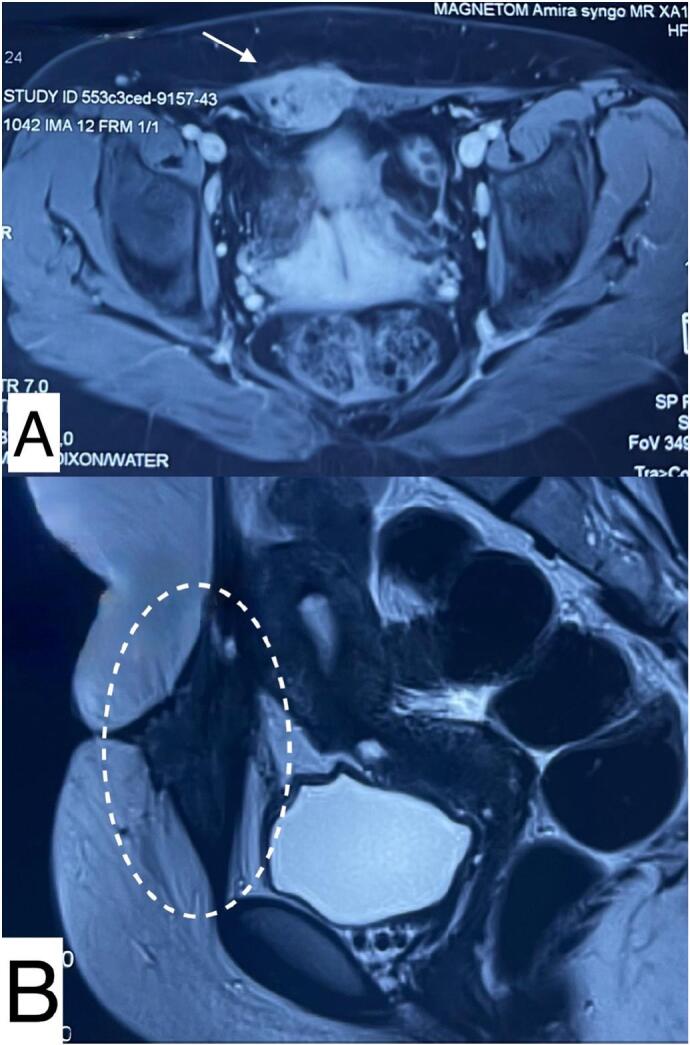
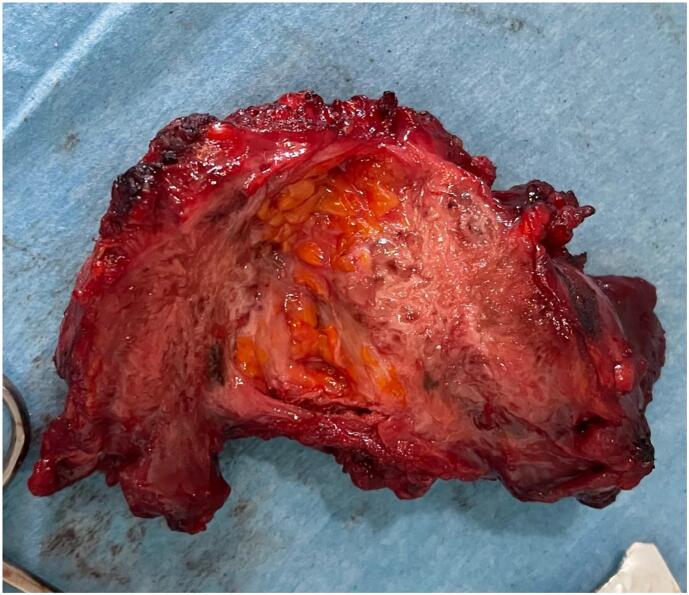
Case presentation: A 26 years old patient presents with recurring pain and swelling of a Pfannenstiel scar 6 years after a caesarean section. Physical examination revealed a firm tender subcutaneous nodule that appeared at MRI as a heterogenous parietal mass infiltrating the rectus abdominis muscles. The patient underwent a wide excision of the nodule.
Discussion: Parietal endometriosis can be the cause of debilitating scar pain even in patients with no history of deep endometriosis. It presents as firm parietal nodule that can become large and infiltrative if left untreated. Diagnosis is purely histological. Surgery remains the treatment of choice and requires a wide excision.
Conclusion: Parietal endometriosis, potentially more common due to rising number of caesarean sections, should be considered with persistent scar pain. Surgery is the preferred treatment, offering a conclusive diagnosis.
Keywords: Caesarean section scar; Catamenial pain; Nodule; Parietal endometriosis; Wide excision.
Copyright © 2024 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors declare that they have no competing interests relevant to the content of this article.
Figures

Similar articles
-
Extrapelvic endometriosis located individually in the rectus abdominis muscle: a rare cause of chronic pelvic pain (a case report).Pan Afr Med J. 2022 Jul 29;42:242. doi: 10.11604/pamj.2022.42.242.36325. eCollection 2022. Pan Afr Med J. 2022. PMID: 36303823 Free PMC article.
-
Skin Endometriosis at the Caesarean Section Scar: A Case Report and Review of the Literature.Cureus. 2018 Jan 13;10(1):e2063. doi: 10.7759/cureus.2063. Cureus. 2018. PMID: 29545986 Free PMC article.
-
Abdominal Wall Endometriosis at the Cesarean Section Scar.Pril (Makedon Akad Nauk Umet Odd Med Nauki). 2023 Dec 18;44(3):121-126. doi: 10.2478/prilozi-2023-0055. Print 2023 Dec 1. Pril (Makedon Akad Nauk Umet Odd Med Nauki). 2023. PMID: 38109456
-
Endometriosis-associated clear cell carcinoma arising in caesarean section scar: a case report and review of the literature.World J Surg Oncol. 2016 Dec 3;14(1):300. doi: 10.1186/s12957-016-1054-7. World J Surg Oncol. 2016. PMID: 27912770 Free PMC article. Review.
-
[Parietal endometriosis on caesarean section scar].Rev Prat. 2019 Apr;69(4):429-431. Rev Prat. 2019. PMID: 31626501 Review. French.
References
Publication types
LinkOut - more resources
Full Text Sources
