

Use of point-of-care ultrasound in rural British Columbia: Scale, training, and barriers
- PMID: 38383018
- PMCID: PMC11271830
- DOI: 10.46747/cfp.7002109
Use of point-of-care ultrasound in rural British Columbia: Scale, training, and barriers
Abstract
Objective: To determine the scale and scope of use of point-of-care ultrasound (POCUS) in rural British Columbia (BC).
Design: Online survey.
Setting: Rural BC.
Participants: Physicians practising in rural BC communities.
Main outcome measures: Practitioner demographic and practice characteristics, locations and frequency of POCUS use, POCUS education and training, and practitioner attitudes about and barriers to POCUS use.
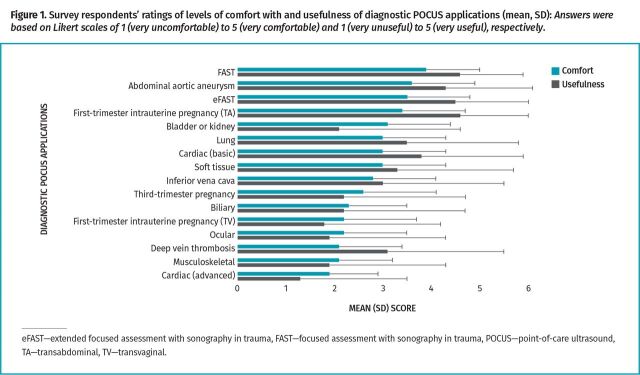
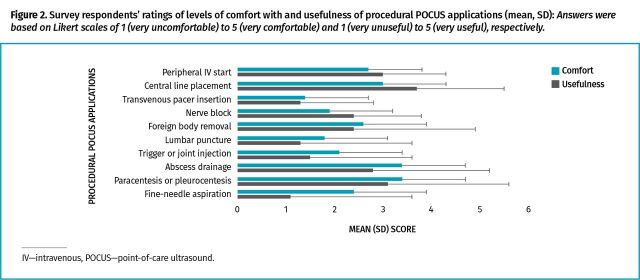
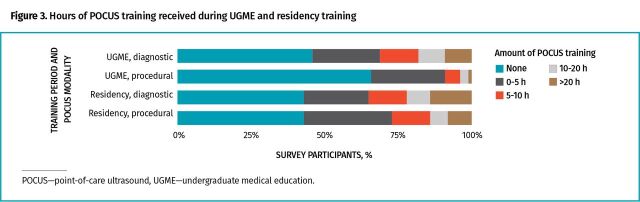
Results: Two hundred twenty-seven surveys were completed in fall 2021, corresponding to a response rate of 11.9% of all rural practitioners in BC. A total of 52.1% of respondents worked in communities with less than 10,000 people, while 24.9% had practices with relatively large proportions of Indigenous patients (more than 20% of the practice population). Respondents reported ease of access to local POCUS devices, with use highest in emergency departments (87.2%) followed by ambulatory care clinic (54.7%) and inpatient (50.3%) settings. Use of POCUS influenced clinical decision making in half the occasions in which it was employed, including a range of diagnostic and procedural applications. Barriers to use included lack of training, limited time to perform POCUS scans, and absence of image review or consultative support. Needed support for POCUS identified by respondents included real-time image acquisition advice and funding for both device acquisition and training. Recommendations for including POCUS training in undergraduate and residency education were strongly supported.
Conclusion: Use of POCUS in BC is expanding in frequency, scope, and scale in practices serving rural areas and in rural communities with large Indigenous populations, with practitioners reporting important improvements in clinical care as a result. Future research could help improve systemic support for POCUS use, guide needed curriculum changes in medical school and postgraduate training, and be used to inform continuing professional development needs.
Objectif: Déterminer l’étendue et la portée de l’utilisation de l’échographie au point de service (EGPS) dans des milieux ruraux de la Colombie-Britannique (C.-B.).
Type d’étude: Un sondage en ligne.
Contexte: Des milieux ruraux de la C.-B.
Participants: Des médecins qui pratiquent dans des communautés rurales de la C.-B.
Principaux paramètres à l’étude: Les caractéristiques démographiques des médecins et la nature de leur pratique, l’emplacement et la fréquence de l’EGPS, l’éducation et la formation relatives à l’EGPS, les attitudes des médecins concernant le recours à l’EGPS et les obstacles à son utilisation.
Résultats: À l’automne de 2021, 227 sondages ont été remplis, ce qui correspond à un taux de réponse de 11,9 % de tous les médecins ruraux en C.-B. Dans l’ensemble, 52,1 % des répondants travaillaient dans des communautés de moins de 10 000 habitants, alors que 24,9 % avaient des pratiques comportant des proportions relativement importantes de patients autochtones (plus de 20 % de la population de la pratique). Les répondants ont signalé une facilité d’accès aux appareils locaux d’EGPS, dont l’accès le plus fréquent se situait dans les départements d’urgence (87,2 %), suivis par les cliniques de soins ambulatoires (54,7 %) et les milieux hospitaliers (50,3 %). L’utilisation de l’EGPS avait influé sur la prise de décision clinique dans la moitié des cas où elle avait été utilisée, notamment dans une diversité d’applications diagnostiques et procédurales. Au nombre des obstacles à son utilisation figuraient le manque de formation, le temps limité pour effectuer les échographies, et l’absence de soutien pour l’analyse de l’imagerie ou de soutien consultatif. Les soutiens nécessaires à l’EGPS qu’ont cernés les répondants incluaient des conseils sur l’acquisition d’images en temps réel, et du financement pour l’acquisition des appareils et la formation. La recommandation d’intégrer la formation sur l’EGPS dans l’éducation prédoctorale et postdoctorale a reçu un fort appui.
Conclusion: L’utilisation de l’EGPS s’accroît en fréquence, en portée et en étendue dans les pratiques desservant des régions rurales et dans les communautés rurales qui ont d’importantes populations autochtones, et les médecins ont signalé des améliorations considérables aux soins cliniques qui en ont découlé. Des recherches futures pourraient contribuer à améliorer le soutien systémique à l’utilisation de l’EGPS, à orienter les changements nécessaires aux cursus durant les études de médecine et la formation postdoctorale, et à détermine les besoins en développement professionnel continu.
Copyright © 2024 the College of Family Physicians of Canada.
Figures
Similar articles
-
The assessment of point-of-care ultrasound (POCUS) in residency: the benefits of a four-year longitudinally integrated curriculum.J Osteopath Med. 2025 Jan 8;125(3):119-126. doi: 10.1515/jom-2024-0046. eCollection 2025 Mar 1. J Osteopath Med. 2025. PMID: 39764717
-
Rural family physician use of point-of-care ultrasonography: experiences of primary care providers in British Columbia, Canada.BMC Prim Care. 2023 Sep 8;24(1):183. doi: 10.1186/s12875-023-02128-z. BMC Prim Care. 2023. PMID: 37684568 Free PMC article.
-
Barriers to point-of-care ultrasound use in rural emergency departments.CJEM. 2016 Nov;18(6):475-479. doi: 10.1017/cem.2016.337. Epub 2016 Jul 25. CJEM. 2016. PMID: 27452408 Review.
-
A majority of rural emergency departments in the province of Quebec use point-of-care ultrasound: a cross-sectional survey.BMC Emerg Med. 2015 Dec 11;15:36. doi: 10.1186/s12873-015-0063-0. BMC Emerg Med. 2015. PMID: 26655376 Free PMC article.
-
Barriers to learning and performing point-of-care ultrasound (POCUS): An integrative review.J Prof Nurs. 2024 Sep-Oct;54:54-62. doi: 10.1016/j.profnurs.2024.06.007. Epub 2024 Jun 24. J Prof Nurs. 2024. PMID: 39266108 Review.
Cited by
-
In every disadvantage there is an advantage: Drug shortages and other challenges in family medicine.Can Fam Physician. 2024 Feb;70(2):79. doi: 10.46747/cfp.700279. Can Fam Physician. 2024. PMID: 38383017 Free PMC article. No abstract available.
References
-
- Kendall JL, Hoffenberg SR, Smith RS.. History of emergency and critical care ultrasound: the evolution of a new imaging paradigm. Crit Care Med 2007;35(5 Suppl):S126-30. - PubMed
-
- McCormick TJ, Clarke Miller E, Chen R, Naik VN.. Acquiring and maintaining point-of-care ultrasound (POCUS) competence for anesthesiologists. Can J Anaesth 2018;65(4):427-36. Epub 2018 Jan 11. - PubMed
-
- Point-of-care ultrasound: recommended curriculum guidelines for family medicine residents. Leawood, KS: American Academy of Family Physicians; 2021. Available from: https://www.aafp.org/dam/AAFP/documents/medical_education_residency/prog.... Accessed 2024 Jan 19.
-
- Díaz-Gómez JL, Mayo PH, Koenig SJ.. Point-of-care ultrasonography. N Engl J Med 2021;385(17):1593-602. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical