

Genotype-specific spinal cord damage in spinocerebellar ataxias: an ENIGMA-Ataxia study
- PMID: 38383154
- PMCID: PMC11187354
- DOI: 10.1136/jnnp-2023-332696
Genotype-specific spinal cord damage in spinocerebellar ataxias: an ENIGMA-Ataxia study
Abstract
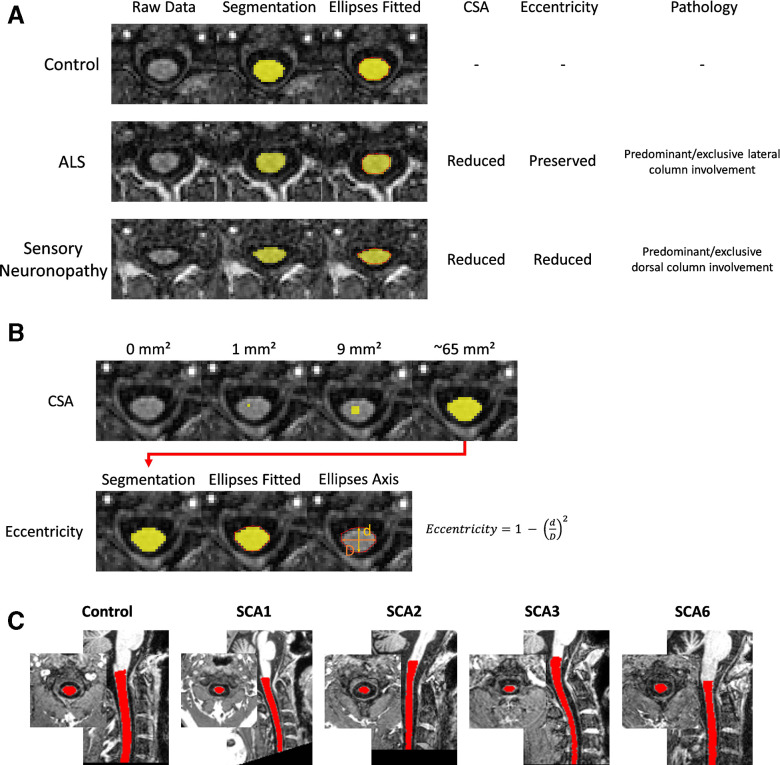
Background: Spinal cord damage is a feature of many spinocerebellar ataxias (SCAs), but well-powered in vivo studies are lacking and links with disease severity and progression remain unclear. Here we characterise cervical spinal cord morphometric abnormalities in SCA1, SCA2, SCA3 and SCA6 using a large multisite MRI dataset.
Methods: Upper spinal cord (vertebrae C1-C4) cross-sectional area (CSA) and eccentricity (flattening) were assessed using MRI data from nine sites within the ENIGMA-Ataxia consortium, including 364 people with ataxic SCA, 56 individuals with preataxic SCA and 394 nonataxic controls. Correlations and subgroup analyses within the SCA cohorts were undertaken based on disease duration and ataxia severity.
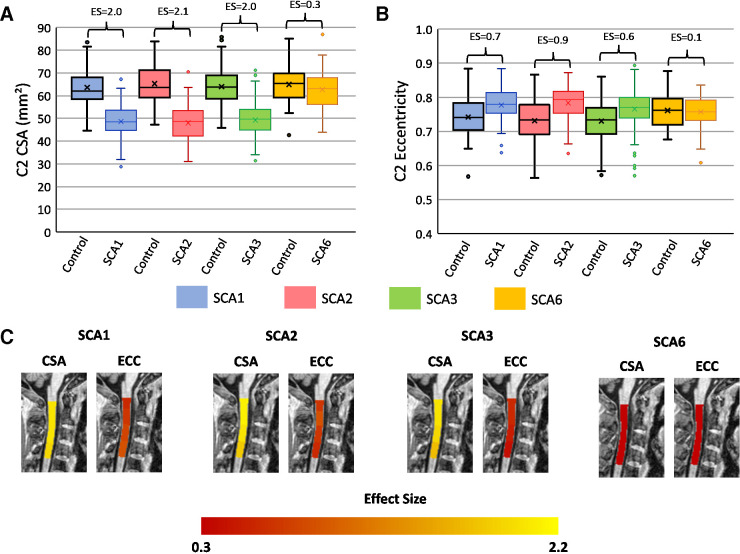
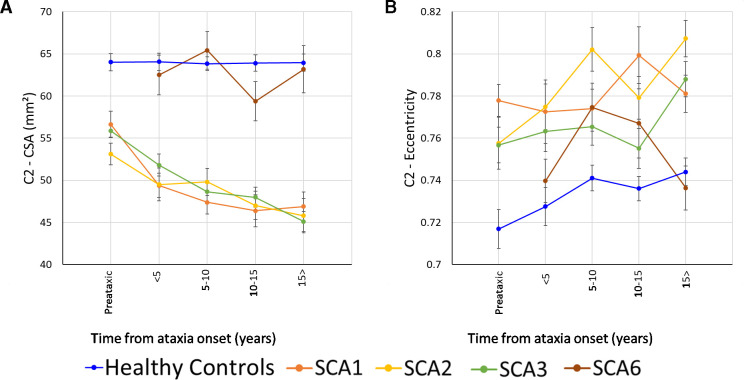
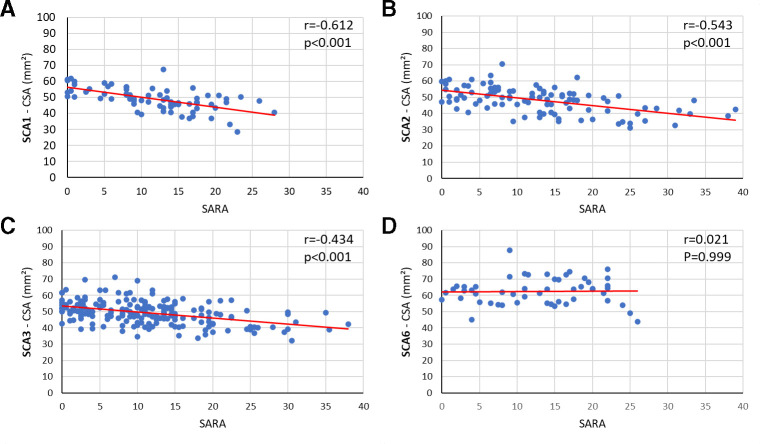
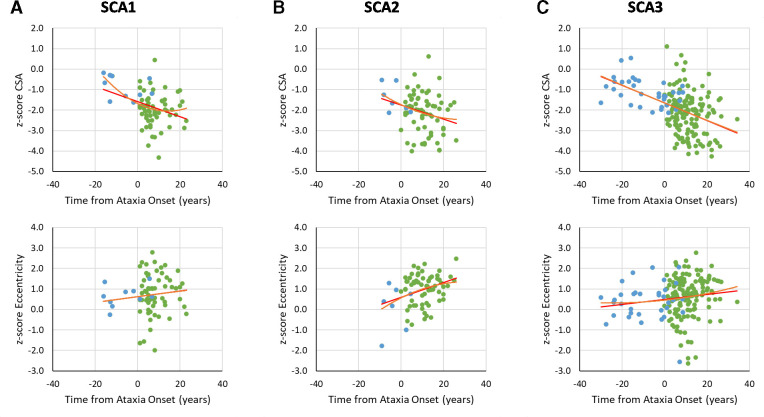
Results: Individuals in the ataxic stage of SCA1, SCA2 and SCA3, relative to non-ataxic controls, had significantly reduced CSA and increased eccentricity at all examined levels. CSA showed large effect sizes (d>2.0) and correlated with ataxia severity (r<-0.43) and disease duration (r<-0.21). Eccentricity correlated only with ataxia severity in SCA2 (r=0.28). No significant spinal cord differences were evident in SCA6. In preataxic individuals, CSA was significantly reduced in SCA2 (d=1.6) and SCA3 (d=1.7), and the SCA2 group also showed increased eccentricity (d=1.1) relative to nonataxic controls. Subgroup analyses confirmed that CSA and eccentricity are abnormal in early disease stages in SCA1, SCA2 and SCA3. CSA declined with disease progression in all, whereas eccentricity progressed only in SCA2.
Conclusions: Spinal cord abnormalities are an early and progressive feature of SCA1, SCA2 and SCA3, but not SCA6, which can be captured using quantitative MRI.
Keywords: MRI; cerebellar ataxia; image analysis; neurogenetics.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: TJRR, FC, ARMM, JLP, OB, BKM, IHH, AD, DT, SLG, ID, IA, GO, CM, LN, AN, MG, LC, HAGT, SEO, CRHR, JFR, FM, AD, BW, JG, MS, PMT, SIT: none. The authors declare no competing interests. KR received honoraria for presentations or advisory boards from Biogen and Roche as well as clinical trial grants from Pfizer, Merck, Minoryx, Biogen and Roche. BB is cofounder, shareholder and CTO of AIRAmed GmbH. CL received research grants from Minoryx Therapeutics and research support from Biogen Inc.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous