

The effectiveness of hysteroscopy for the treatment of cesarean scar pregnancy: a retrospective cohort study
- PMID: 38383385
- PMCID: PMC10880367
- DOI: 10.1186/s12884-024-06344-y
The effectiveness of hysteroscopy for the treatment of cesarean scar pregnancy: a retrospective cohort study
Abstract
Background: Cesarean scar pregnancy (CSP) is a long-term complication of cesarean section characterized by the localization of a subsequent gestational sac within the scar area or niche developed as a result of a previous cesarean section. Its incidence has increased substantially because of the high global cesarean section rate in recent decades. Several surgical and drug treatments exist for this condition; however, there is currently no optimal treatment. This study compared the effectiveness of direct hysteroscopic removal of the gestational tissue and hysteroscopy combined with vacuum suction for the treatment of CSP.
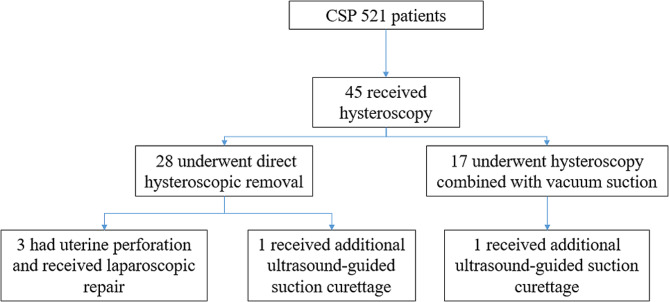
Methods: From 2017 to 2023, 521 patients were diagnosed with CSP at our hospital. Of these patients, 45 underwent hysteroscopy. Among them, 28 underwent direct hysteroscopic removal (hysteroscopic removal group) and 17 underwent hysteroscopy combined with vacuum suction (hysteroscopic suction group). The clinical characteristics and outcomes of the hysteroscopic removal group and hysteroscopic suction group were analyzed.
Results: Among the 45 patients, the amount of bleeding and hospitalization cost were significantly higher in the hysteroscopic removal group than in the hysteroscopic suction group (33.8 mL vs. 9.9 mL, P < 0.001; and 8744.0 yuan vs. 5473.8 yuan, P < 0.001; respectively). The operation time and duration of hospitalization were significantly longer in the hysteroscopic removal group than in the hysteroscopic suction group (61.4 min vs. 28.2 min, P < 0.001; and 3.8 days vs. 2.4 days, P = 0.026; respectively). Three patients in the hysteroscopic removal group had uterine perforation and received laparoscopic repair during operation. No complications occurred in the hysteroscopic suction group. One patient in the hysteroscopic removal group received ultrasound-guided suction curettage due to postoperative moderate vaginal bleeding, and one patient in the hysteroscopic suction group received ultrasound-guided suction curettage due to postoperative gestational residue and elevated serum beta-human chorionic gonadotropin levels. Reproductive function was preserved in all patients.
Conclusions: Hysteroscopy is an effective method for treating CSP. Compared with direct hysteroscopic removal, hysteroscopy combined with vacuum suction is more suitable for CSP. However, multicenter prospective studies with large sample sizes are required for verification of these findings.
Keywords: Cesarean scar pregnancy; Direct gestational tissue removal; Hysteroscopy; Serum β-hCG; Vacuum suction.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Management of persistent caesarean scar pregnancy after curettage treatment failure.BMC Pregnancy Childbirth. 2017 Jul 1;17(1):208. doi: 10.1186/s12884-017-1395-4. BMC Pregnancy Childbirth. 2017. PMID: 28666477 Free PMC article.
-
Conservative cesarean scar pregnancy treatment: local methotrexate injection followed by hysteroscopic removal with hysteroscopic tissue removal system.Fertil Steril. 2021 Nov;116(5):1417-1419. doi: 10.1016/j.fertnstert.2021.06.034. Epub 2021 Jul 18. Fertil Steril. 2021. PMID: 34289934
-
A comparison between laparoscopy and hysteroscopy approach in treatment of cesarean scar pregnancy.Medicine (Baltimore). 2020 Oct 23;99(43):e22845. doi: 10.1097/MD.0000000000022845. Medicine (Baltimore). 2020. PMID: 33120815 Free PMC article.
-
Hysteroscopy and suction evacuation of cesarean scar pregnancies: a case report and review.J Obstet Gynaecol Res. 2014 Mar;40(3):853-7. doi: 10.1111/jog.12260. Epub 2013 Dec 10. J Obstet Gynaecol Res. 2014. PMID: 24320609 Review.
-
Management of cesarean scar pregnancy with suction curettage: a report of four cases and review of the literature.Arch Gynecol Obstet. 2014 Jun;289(6):1171-5. doi: 10.1007/s00404-014-3143-6. Epub 2014 Jan 25. Arch Gynecol Obstet. 2014. PMID: 24464347 Review.
Cited by
-
Immediate Changes in the Elasticity of Tissue and the Pain Pressure Threshold in Cesarean Scar Tissue After a Vacuum Intervention: An Open Clinical Trial.Biomedicines. 2025 Feb 21;13(3):557. doi: 10.3390/biomedicines13030557. Biomedicines. 2025. PMID: 40149534 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
