

PARP1-targeted fluorescence molecular endoscopy as novel tool for early detection of esophageal dysplasia and adenocarcinoma
- PMID: 38383387
- PMCID: PMC10880256
- DOI: 10.1186/s13046-024-02963-7
PARP1-targeted fluorescence molecular endoscopy as novel tool for early detection of esophageal dysplasia and adenocarcinoma
Abstract
Background: Esophageal cancer is one of the 10 most common cancers worldwide and its incidence is dramatically increasing. Despite some improvements, the current surveillance protocol with white light endoscopy and random untargeted biopsies collection (Seattle protocol) fails to diagnose dysplastic and cancerous lesions in up to 50% of patients. Therefore, new endoscopic imaging technologies in combination with tumor-specific molecular probes are needed to improve early detection. Herein, we investigated the use of the fluorescent Poly (ADP-ribose) Polymerase 1 (PARP1)-inhibitor PARPi-FL for early detection of dysplastic lesions in patient-derived organoids and transgenic mouse models, which closely mimic the transformation from non-malignant Barrett's Esophagus (BE) to invasive esophageal adenocarcinoma (EAC).
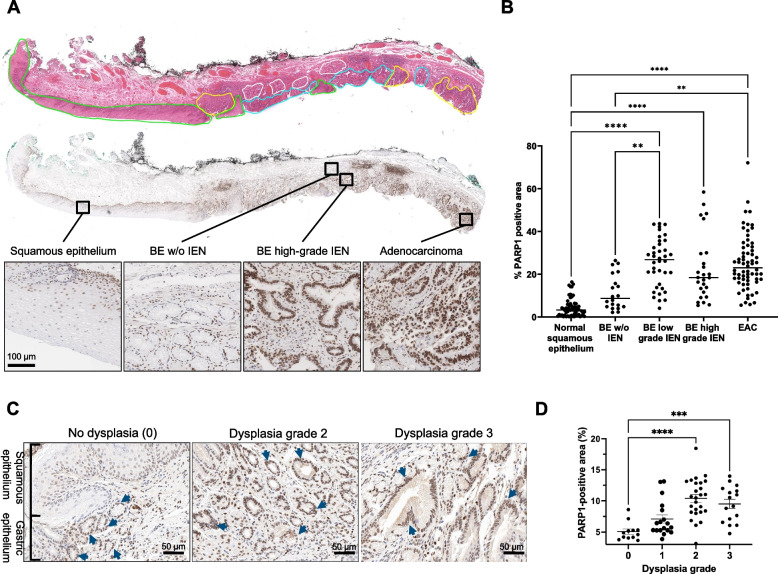
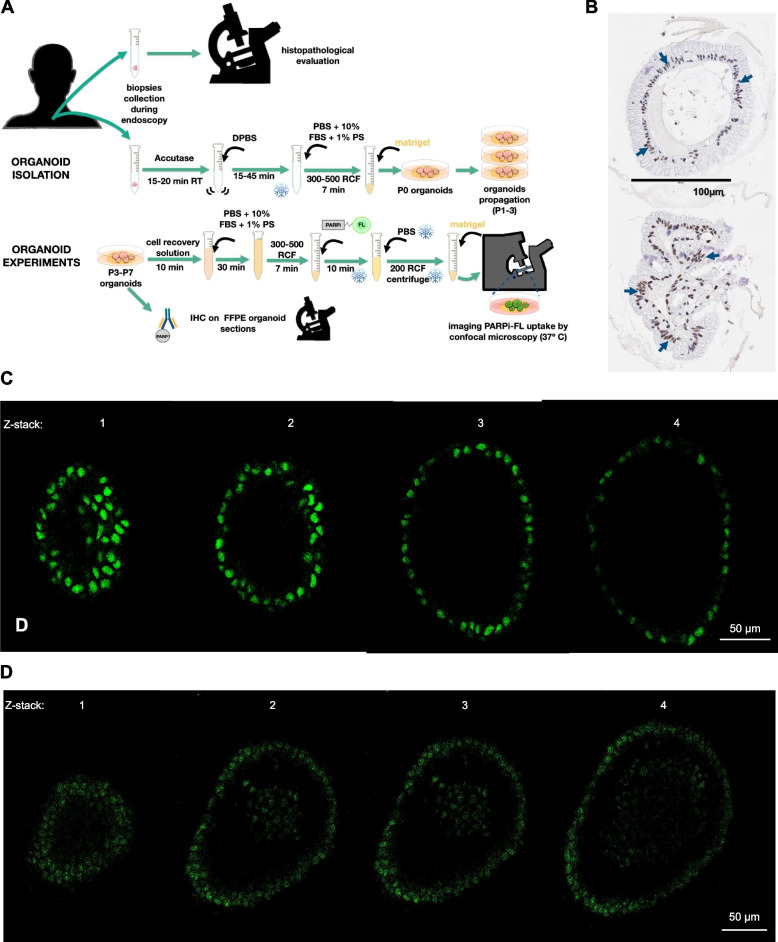
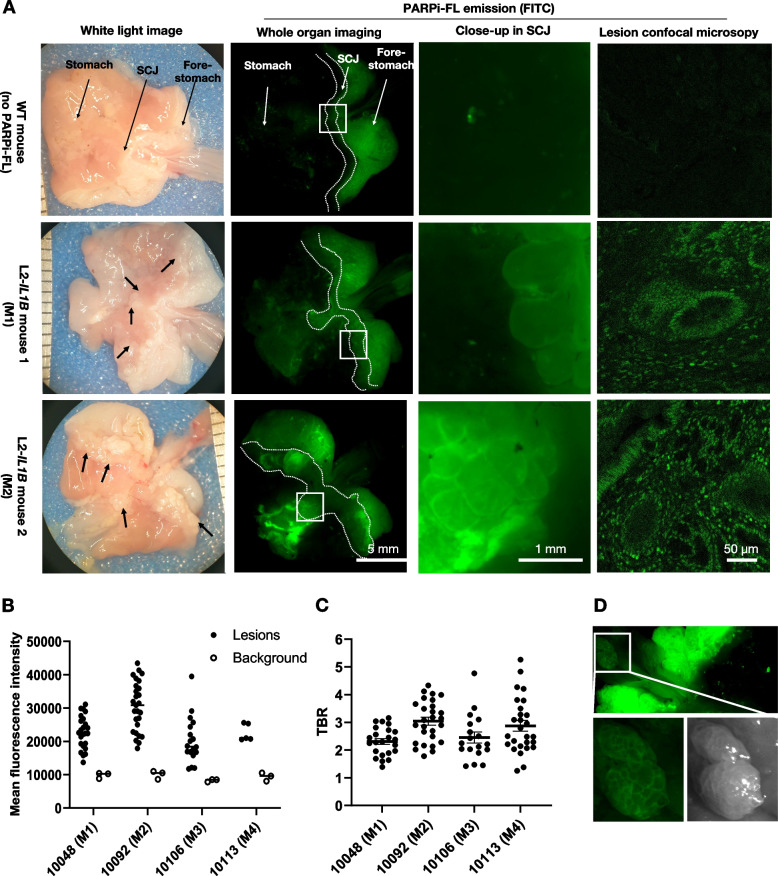
Methods: We determined PARP1 expression via immunohistochemistry (IHC) in human biospecimens and mouse tissues. We also assessed PARPi-FL uptake in patient- and mouse-derived organoids. Following intravenous injection of 75 nmol PARPi-FL/mouse in L2-IL1B (n = 4) and L2-IL1B/IL8Tg mice (n = 12), we conducted fluorescence molecular endoscopy (FME) and/or imaged whole excised stomachs to assess PARPi-FL accumulation in dysplastic lesions. L2-IL1B/IL8Tg mice (n = 3) and wild-type (WT) mice (n = 2) without PARPi-FL injection served as controls. The imaging results were validated by confocal microscopy and IHC of excised tissues.
Results: IHC on patient and murine tissue revealed similar patterns of increasing PARP1 expression in presence of dysplasia and cancer. In human and murine organoids, PARPi-FL localized to PARP1-expressing epithelial cell nuclei after 10 min of incubation. Injection of PARPi-FL in transgenic mouse models of BE resulted in the successful detection of lesions via FME, with a mean target-to-background ratio > 2 independently from the disease stage. The localization of PARPi-FL in the lesions was confirmed by imaging of the excised stomachs and confocal microscopy. Without PARPi-FL injection, identification of lesions via FME in transgenic mice was not possible.
Conclusion: PARPi-FL imaging is a promising approach for clinically needed improved detection of dysplastic and malignant EAC lesions in patients with BE. Since PARPi-FL is currently evaluated in a phase 2 clinical trial for oral cancer detection after topical application, clinical translation for early detection of dysplasia and EAC in BE patients via FME screening appears feasible.
Keywords: Animal Models; Dysplasia; Esophageal Adenocarcinoma; Fluorescence Imaging; Fluorescence Molecular Endoscopy; PARP1.
© 2024. The Author(s).
Conflict of interest statement
S.K. is a shareholder of Summit Biomedical Imaging, LLC. SK is a co- inventor on PCT application WO2016164771. V.N. is a founder and equity owner of sThesis GmbH, iThera Medical GmbH, Spear UG and I3 Inc. All other authors have no relevant conflict of interest to declare.
Figures


Similar articles
-
Targeting c-MET for Endoscopic Detection of Dysplastic Lesions within Barrett's Esophagus Using EMI-137 Fluorescence Imaging.Clin Cancer Res. 2025 Jan 6;31(1):98-109. doi: 10.1158/1078-0432.CCR-24-1522. Clin Cancer Res. 2025. PMID: 39513952 Free PMC article.
-
Targeted Hsp70 fluorescence molecular endoscopy detects dysplasia in Barrett's esophagus.Eur J Nucl Med Mol Imaging. 2022 May;49(6):2049-2063. doi: 10.1007/s00259-021-05582-y. Epub 2021 Dec 9. Eur J Nucl Med Mol Imaging. 2022. PMID: 34882260 Free PMC article.
-
Notch Signaling Mediates Differentiation in Barrett's Esophagus and Promotes Progression to Adenocarcinoma.Gastroenterology. 2020 Aug;159(2):575-590. doi: 10.1053/j.gastro.2020.04.033. Epub 2020 Apr 20. Gastroenterology. 2020. PMID: 32325086 Free PMC article.
-
Chromoendoscopy and magnification endoscopy for diagnosing esophageal cancer and dysplasia.Thorac Surg Clin. 2004 Feb;14(1):87-94. doi: 10.1016/S1547-4127(04)00042-8. Thorac Surg Clin. 2004. PMID: 15382312 Review.
-
AGA Clinical Practice Update on Endoscopic Treatment of Barrett's Esophagus With Dysplasia and/or Early Cancer: Expert Review.Gastroenterology. 2020 Feb;158(3):760-769. doi: 10.1053/j.gastro.2019.09.051. Epub 2019 Nov 12. Gastroenterology. 2020. PMID: 31730766 Review.
Cited by
-
PARP-1 as a novel target in endocrine-resistant breast cancer.J Exp Clin Cancer Res. 2025 Jun 16;44(1):175. doi: 10.1186/s13046-025-03441-4. J Exp Clin Cancer Res. 2025. PMID: 40518539 Free PMC article.
-
Targeting c-MET for Endoscopic Detection of Dysplastic Lesions within Barrett's Esophagus Using EMI-137 Fluorescence Imaging.Clin Cancer Res. 2025 Jan 6;31(1):98-109. doi: 10.1158/1078-0432.CCR-24-1522. Clin Cancer Res. 2025. PMID: 39513952 Free PMC article.
References
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
