

The SEE-IT Trial: emergency medical services Streaming Enabled Evaluation In Trauma: a feasibility randomised controlled trial
- PMID: 38383402
- PMCID: PMC10883301
- DOI: 10.1186/s13049-024-01179-0
The SEE-IT Trial: emergency medical services Streaming Enabled Evaluation In Trauma: a feasibility randomised controlled trial
Abstract
Background: Use of bystander video livestreaming from scene to Emergency Medical Services (EMS) is becoming increasingly common to aid decision making about the resources required. Possible benefits include earlier, more appropriate dispatch and clinical and financial gains, but evidence is sparse.
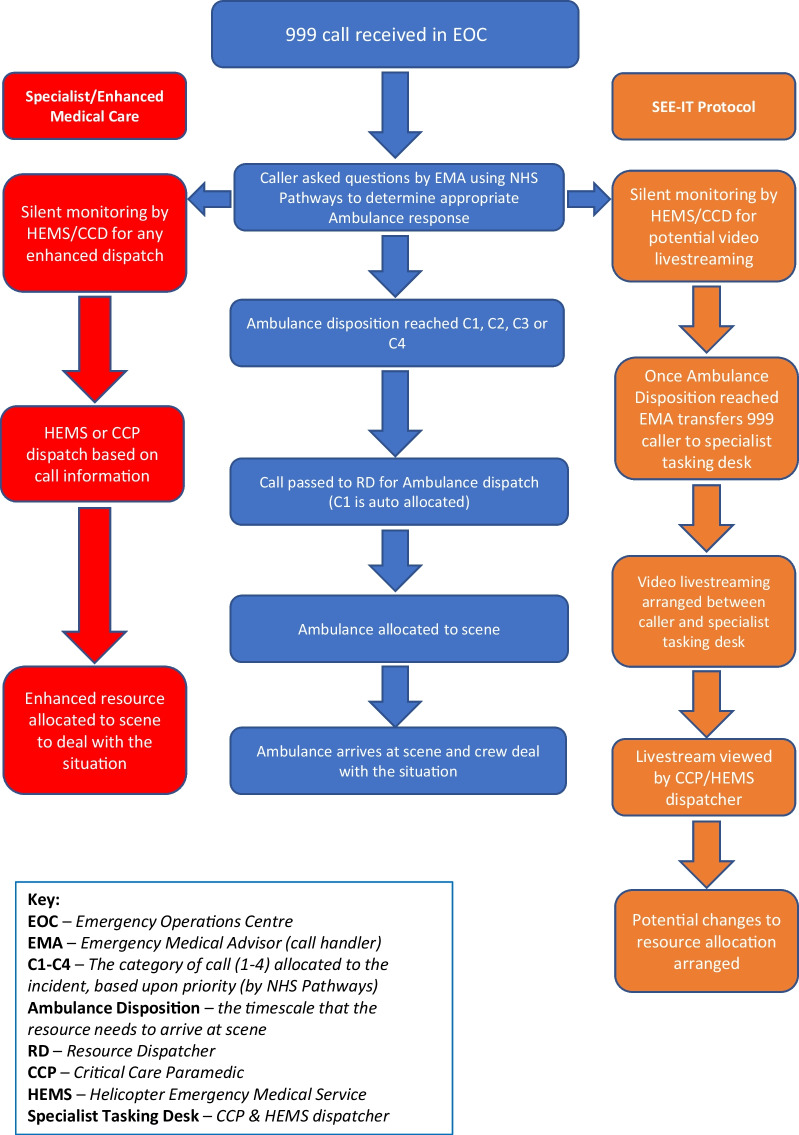
Methods: A feasibility randomised controlled trial with an embedded process evaluation and exploratory economic evaluation where working shifts during six trial weeks were randomised 1:1 to use video livestreaming during eligible trauma incidents (using GoodSAM Instant-On-Scene) or standard care only. Pre-defined progression criteria were: (1) ≥ 70% callers (bystanders) with smartphones agreeing and able to activate live stream; (2) ≥ 50% requests to activate resulting in footage being viewed; (3) Helicopter Emergency Medical Services (HEMS) stand-down rate reducing by ≥ 10% as a result of live footage; (4) no evidence of psychological harm in callers or staff/dispatchers. Observational sub-studies included (i) an inner-city EMS who routinely use video livestreaming to explore acceptability in a diverse population; and (ii) staff wellbeing in an EMS not using video livestreaming for comparison to the trial site.
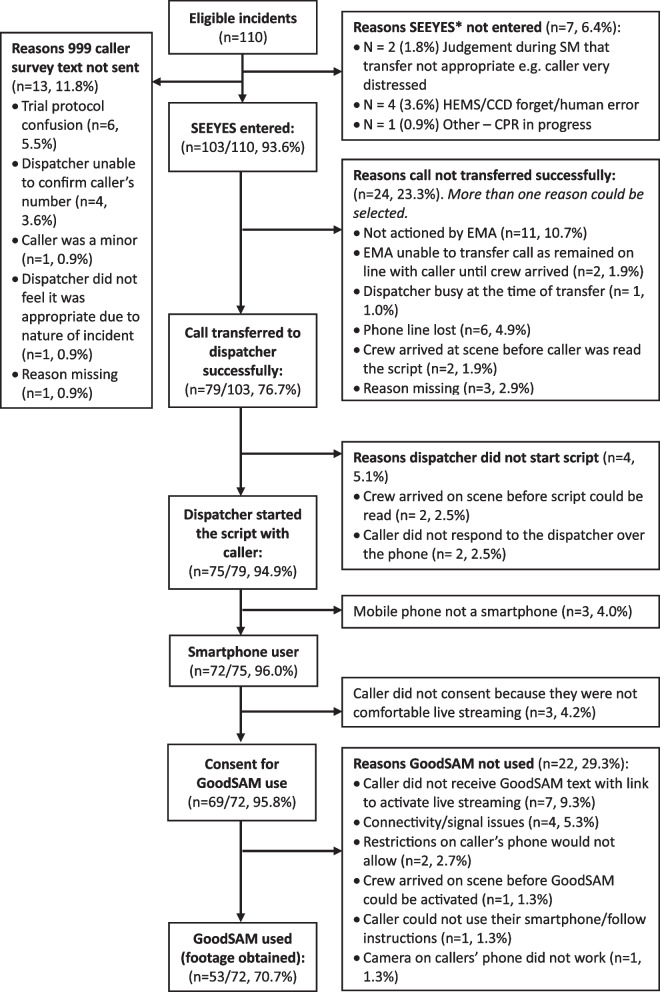
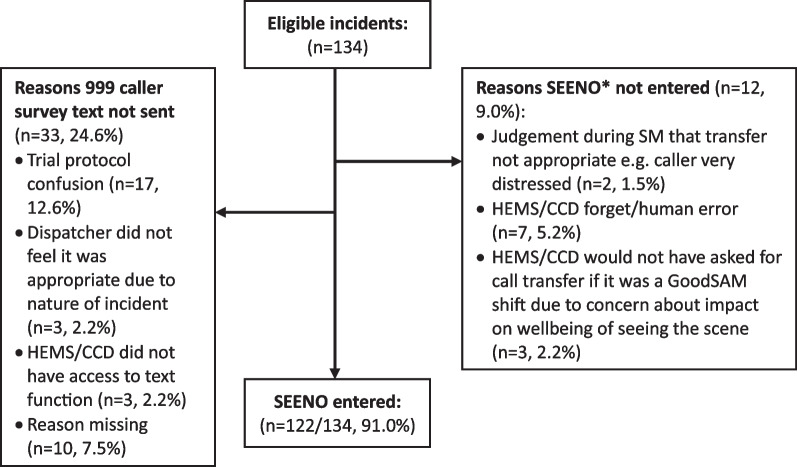
Results: Sixty-two shifts were randomised, including 240 incidents (132 control; 108 intervention). Livestreaming was successful in 53 incidents in the intervention arm. Patient recruitment (to determine appropriateness of dispatch), and caller recruitment (to measure potential harm) were low (58/269, 22% of patients; 4/244, 2% of callers). Two progression criteria were met: (1) 86% of callers with smartphones agreed and were able to activate livestreaming; (2) 85% of requests to activate livestreaming resulted in footage being obtained; and two were indeterminate due to insufficient data: (3) 2/6 (33%) HEMS stand down due to livestreaming; (4) no evidence of psychological harm from survey, observations or interviews, but insufficient survey data from callers or comparison EMS site to be confident. Language barriers and older age were reported in interviews as potential challenges to video livestreaming by dispatchers in the inner-city EMS.
Conclusions: Progression to a definitive RCT is supported by these findings. Bystander video livestreaming from scene is feasible to implement, acceptable to both 999 callers and dispatchers, and may aid dispatch decision-making. Further assessment of unintended consequences, benefits and harm is required.
Trial registration: ISRCTN 11449333 (22 March 2022). https://www.isrctn.com/ISRCTN11449333.
Keywords: Air ambulance; Critical care; Emergency medical dispatch; Emergency medical resource; Emergency medical services; Helicopter emergency medical services; Pre-hospital; Smartphone; Trauma; Video.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Eaton G, Raitt J, Brown S, Parsons V. How appropriate are the data produced by NHS pathways for identifying suitable cases for involvement of enhanced care teams? Br Paramed J. 2017;2(3):16–23. doi: 10.29045/14784726.2017.2.3.16. - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
