

Novel subtypes of severe COVID-19 respiratory failure based on biological heterogeneity: a secondary analysis of a randomized controlled trial
- PMID: 38383504
- PMCID: PMC10882728
- DOI: 10.1186/s13054-024-04819-0
Novel subtypes of severe COVID-19 respiratory failure based on biological heterogeneity: a secondary analysis of a randomized controlled trial
Abstract
Background: Despite evidence associating inflammatory biomarkers with worse outcomes in hospitalized adults with COVID-19, trials of immunomodulatory therapies have met with mixed results, likely due in part to biological heterogeneity of participants. Latent class analysis (LCA) of clinical and protein biomarker data has identified two subtypes of non-COVID acute respiratory distress syndrome (ARDS) with different clinical outcomes and treatment responses. We studied biological heterogeneity and clinical outcomes in a multi-institutional platform randomized controlled trial of adults with severe COVID-19 hypoxemic respiratory failure (I-SPY COVID).
Methods: Clinical and plasma protein biomarker data were analyzed from 400 trial participants enrolled from September 2020 until October 2021 with severe COVID-19 requiring ≥ 6 L/min supplemental oxygen. Seventeen hypothesis-directed protein biomarkers were measured at enrollment using multiplex Luminex panels or single analyte enzyme linked immunoassay methods (ELISA). Biomarkers and clinical variables were used to test for latent subtypes and longitudinal biomarker changes by subtype were explored. A validated parsimonious model using interleukin-8, bicarbonate, and protein C was used for comparison with non-COVID hyper- and hypo-inflammatory ARDS subtypes.
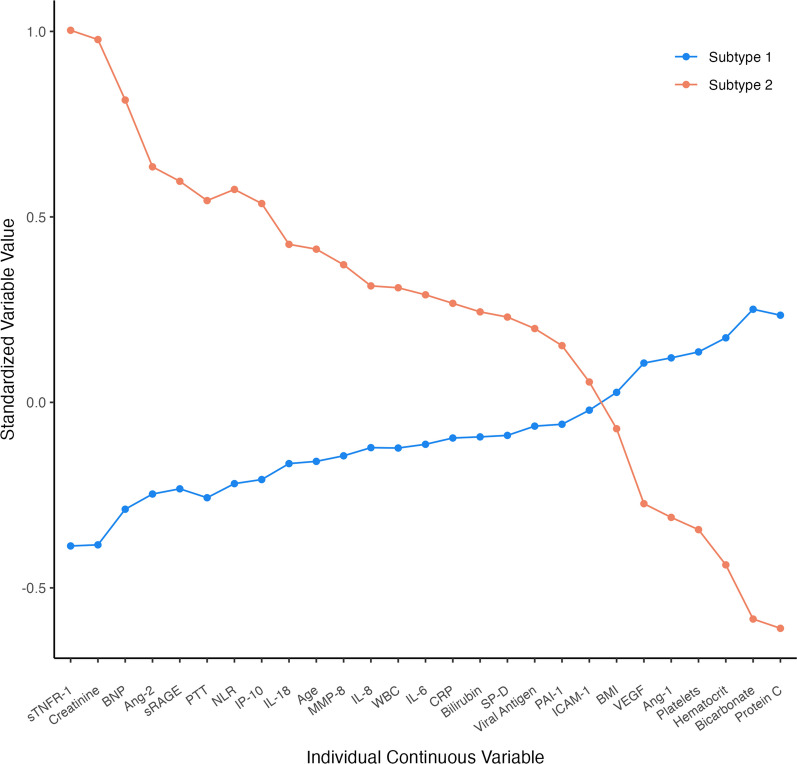
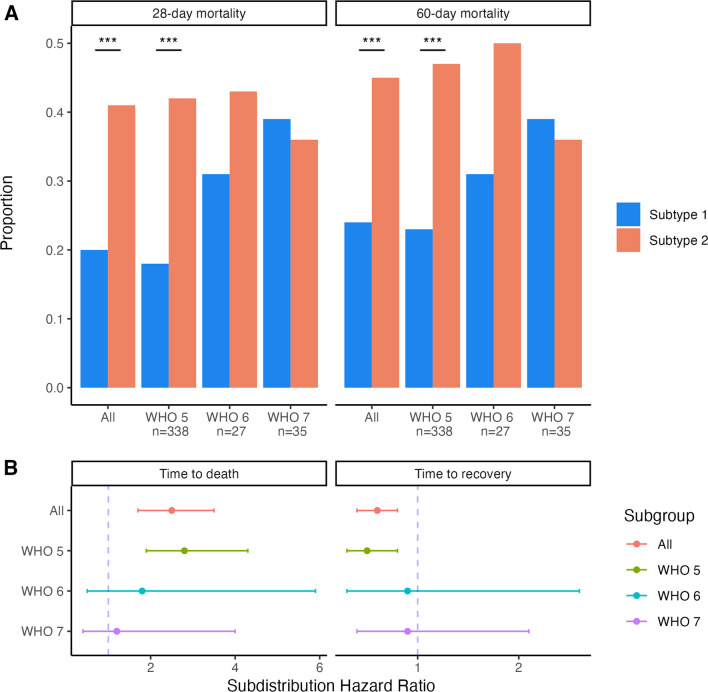
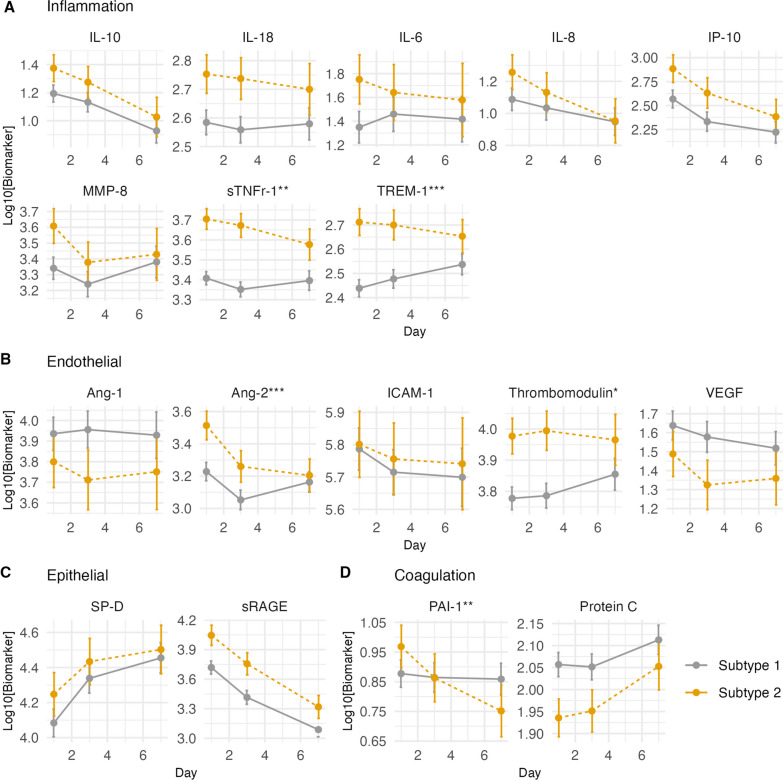
Results: Average participant age was 60 ± 14 years; 67% were male, and 28-day mortality was 25%. At trial enrollment, 85% of participants required high flow oxygen or non-invasive ventilation, and 97% were receiving dexamethasone. Several biomarkers of inflammation (IL-6, IL-8, IL-10, sTNFR-1, TREM-1), epithelial injury (sRAGE), and endothelial injury (Ang-1, thrombomodulin) were associated with 28- and 60-day mortality. Two latent subtypes were identified. Subtype 2 (27% of participants) was characterized by persistent derangements in biomarkers of inflammation, endothelial and epithelial injury, and disordered coagulation and had twice the mortality rate compared with Subtype 1. Only one person was classified as hyper-inflammatory using the previously validated non-COVID ARDS model.
Conclusions: We discovered evidence of two novel biological subtypes of severe COVID-19 with significantly different clinical outcomes. These subtypes differed from previously established hyper- and hypo-inflammatory non-COVID subtypes of ARDS. Biological heterogeneity may explain inconsistent findings from trials of hospitalized patients with COVID-19 and guide treatment approaches.
Keywords: Biological heterogeneity; COVID-19; Hypoxemic respiratory failure; Latent class analysis; Phenotyping; Protein biomarkers.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
