

A multimodal deep learning approach for the prediction of cognitive decline and its effectiveness in clinical trials for Alzheimer's disease
- PMID: 38383536
- PMCID: PMC10882004
- DOI: 10.1038/s41398-024-02819-w
A multimodal deep learning approach for the prediction of cognitive decline and its effectiveness in clinical trials for Alzheimer's disease
Abstract
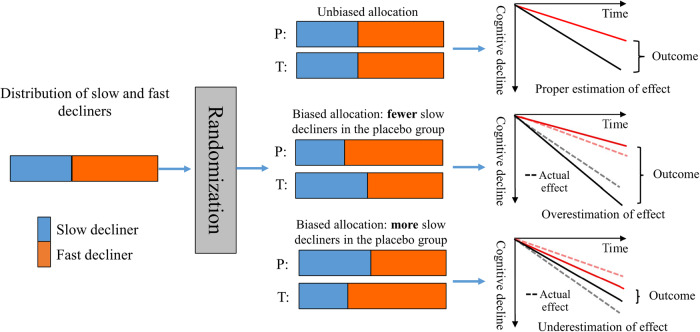
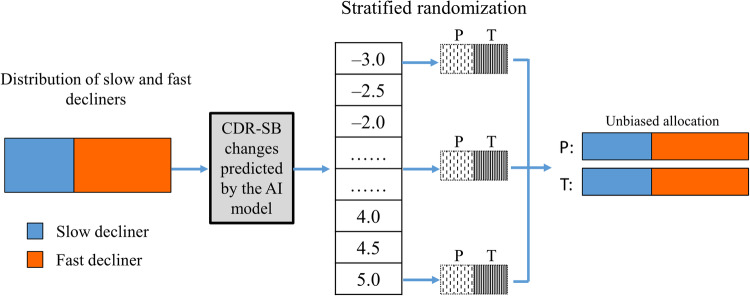
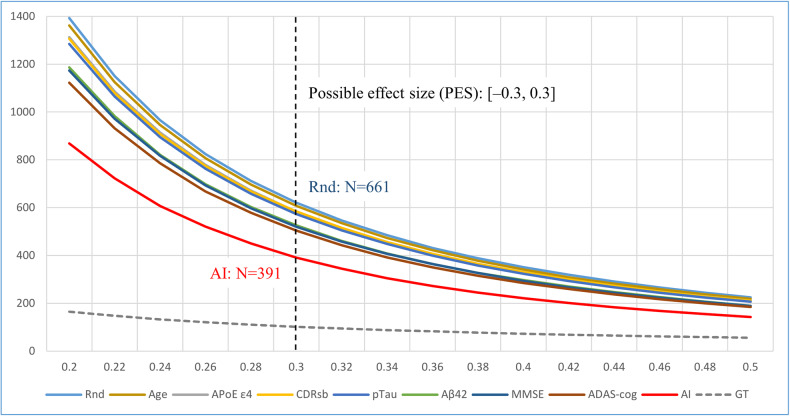
Alzheimer's disease is one of the most important health-care challenges in the world. For decades, numerous efforts have been made to develop therapeutics for Alzheimer's disease, but most clinical trials have failed to show significant treatment effects on slowing or halting cognitive decline. Among several challenges in such trials, one recently noticed but unsolved is biased allocation of fast and slow cognitive decliners to treatment and placebo groups during randomization caused by the large individual variation in the speed of cognitive decline. This allocation bias directly results in either over- or underestimation of the treatment effect from the outcome of the trial. In this study, we propose a stratified randomization method using the degree of cognitive decline predicted by an artificial intelligence model as a stratification index to suppress the allocation bias in randomization and evaluate its effectiveness by simulation using ADNI data set.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures





Similar articles
-
Long-term cognitive decline prediction based on multi-modal data using Multimodal3DSiameseNet: transfer learning from Alzheimer's disease to Parkinson's disease.Int J Comput Assist Radiol Surg. 2023 May;18(5):809-818. doi: 10.1007/s11548-023-02866-6. Epub 2023 Mar 25. Int J Comput Assist Radiol Surg. 2023. PMID: 36964477 Free PMC article.
-
Prediction of fast decline in amyloid positive mild cognitive impairment patients using multimodal biomarkers.Neuroimage Clin. 2019;24:101941. doi: 10.1016/j.nicl.2019.101941. Epub 2019 Jul 19. Neuroimage Clin. 2019. PMID: 31376643 Free PMC article.
-
Deep Learning and Risk Score Classification of Mild Cognitive Impairment and Alzheimer's Disease.J Alzheimers Dis. 2021;80(3):1079-1090. doi: 10.3233/JAD-201438. J Alzheimers Dis. 2021. PMID: 33646166
-
Consensus-based recommendations for the management of rapid cognitive decline due to Alzheimer's disease.Alzheimers Dement. 2017 May;13(5):592-597. doi: 10.1016/j.jalz.2017.01.007. Epub 2017 Feb 24. Alzheimers Dement. 2017. PMID: 28238739
-
Machine learning methods for predicting progression from mild cognitive impairment to Alzheimer's disease dementia: a systematic review.Alzheimers Res Ther. 2021 Sep 28;13(1):162. doi: 10.1186/s13195-021-00900-w. Alzheimers Res Ther. 2021. PMID: 34583745 Free PMC article.
Cited by
-
Attention-driven hybrid deep learning and SVM model for early Alzheimer's diagnosis using neuroimaging fusion.BMC Med Inform Decis Mak. 2025 Jul 1;25(1):219. doi: 10.1186/s12911-025-03073-w. BMC Med Inform Decis Mak. 2025. PMID: 40597079 Free PMC article.
-
Rationale and design of the BeyeOMARKER study: prospective evaluation of blood- and eye-based biomarkers for early detection of Alzheimer's disease pathology in the eye clinic.Alzheimers Res Ther. 2024 Aug 21;16(1):190. doi: 10.1186/s13195-024-01545-1. Alzheimers Res Ther. 2024. PMID: 39169442 Free PMC article.
-
Limitations of Correlation Coefficients in Research on Functional Connectomes and Psychological Processes.Hum Brain Mapp. 2025 Jul;46(10):e70287. doi: 10.1002/hbm.70287. Hum Brain Mapp. 2025. PMID: 40637219 Free PMC article. Review.
-
Regression Trees With Fused Leaves.Stat Med. 2024 Dec 30;43(30):5872-5884. doi: 10.1002/sim.10272. Epub 2024 Nov 20. Stat Med. 2024. PMID: 39567228
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
