

Short-term and mid-term evaluation of three types of minimally invasive lumbar fusion surgery for treatment of L4/L5 degenerative spondylolisthesis
- PMID: 38383595
- PMCID: PMC10881486
- DOI: 10.1038/s41598-024-54970-5
Short-term and mid-term evaluation of three types of minimally invasive lumbar fusion surgery for treatment of L4/L5 degenerative spondylolisthesis
Abstract
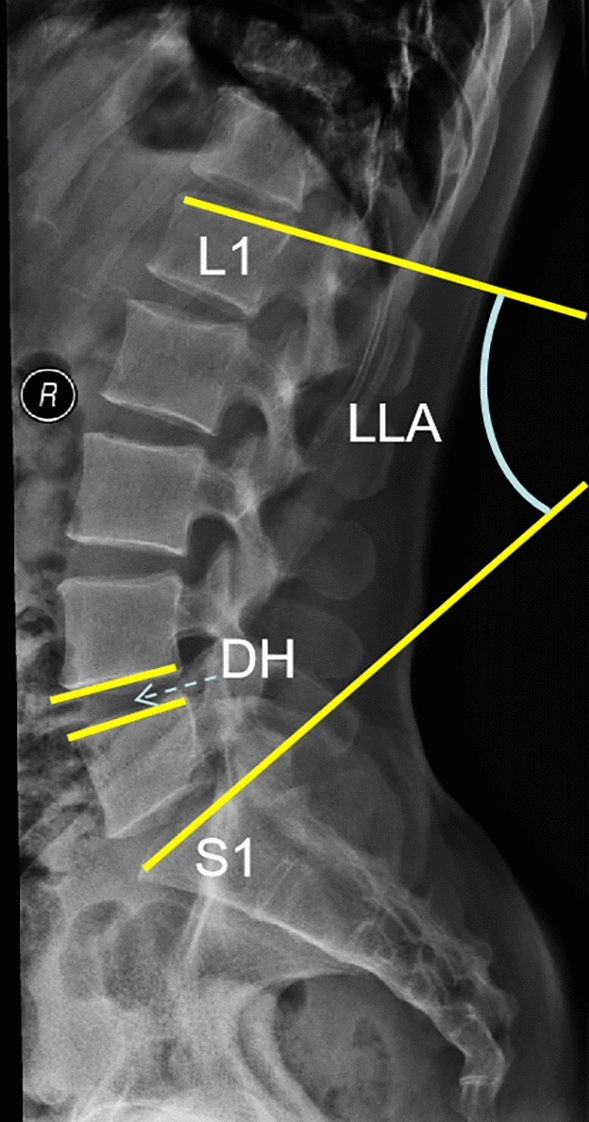
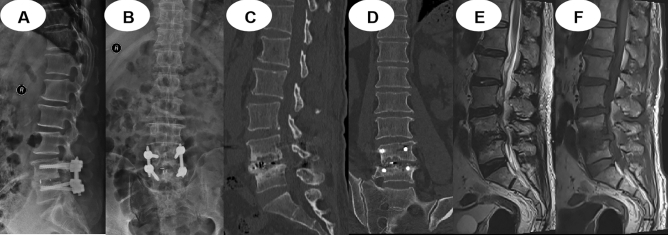
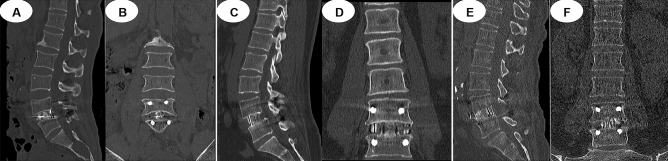
This was a single-centre retrospective study. Minimally invasive techniques for transforaminal lumbar interbody fusion (MIS-TLIF), oblique lumbar interbody fusion (OLIF), and percutaneous endoscopic transforaminal lumbar interbody fusion (Endo-TLIF) have been extensively used for lumbar degenerative diseases. The present study analyses the short-term and mid-term clinical effects of the above three minimally invasive techniques on L4/L5 degenerative spondylolisthesis. In this retrospective study, 98 patients with L4/L5 degenerative spondylolisthesis received MIS-TLIF, 107 received OLIF, and 114 received Endo-TLIF. All patients were followed up for at least one year. We compared patient data, including age, sex, body mass index (BMI), Oswestry disability index (ODI), visual analogue scale of low back pain (VAS-B), visual analogue scale of leg pain (VAS-L), surgical time, blood loss, drainage volume, hospital stay, complications, and neurological status. Moreover, we performed imaging evaluations, including lumbar lordosis angle (LLA), disc height (DH) and intervertebral fusion status. No significant differences were noted in age, sex, BMI, preoperative ODI, preoperative VAS-B, preoperative VAS-L, preoperative LLA, or preoperative DH. Patients who underwent OLIF had significantly decreased blood loss, a lower drainage volume, and a shorter hospital stay than those who underwent MIS-TLIF or Endo-TLIF (P < 0.05). The VAS-B in the OLIF group significantly decreased compared with in the MIS-TLIF and Endo-TLIF groups at 6 and 12 months postoperatively (P < 0.05). The VAS-L in the Endo-TLIF group significantly decreased compared with that in the MIS-TLIF and OLIF groups at 6 months postoperatively (P < 0.05). The ODI in the OLIF group was significantly better than that in the MIS-TLIF and Endo-TLIF groups at 6 months postoperatively (P < 0.05). No statistically significant differences in the incidence of complications and healthcare cost were found among the three groups. Follow-up LLA and DH changes were significantly lower in the OLIF group than in the other groups (P < 0.05). The intervertebral fusion rate was significantly higher in the OLIF group than in the other groups at 6 and 12 months postoperatively (P < 0.05). In conclusion, while MIS-TLIF, OLIF, and Endo-TLIF techniques can effectively treat patients with L4/5 degenerative spondylolisthesis, OLIF has more benefits, including less operative blood loss, a shorter hospital stay, a smaller drainage volume, efficacy for back pain, effective maintenance of lumbar lordosis angle and disc height, and a higher fusion rate. OLIF should be the preferred surgical treatment for patients with L4/5 degenerative spondylolisthesis.
Keywords: Endo-TLIF; Lumbar degenerative spondylolisthesis; MIS-TLIF; OLIF.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Meta-analysis of minimally invasive transforaminal lumbar interbody fusion versus oblique lumbar interbody fusion for treating lumbar degenerative diseases.J Orthop Surg Res. 2024 Dec 30;19(1):891. doi: 10.1186/s13018-024-05422-3. J Orthop Surg Res. 2024. PMID: 39736715 Free PMC article.
-
[Clinical and radiologic comparison between oblique lateral interbody fusion and minimally invasive transforaminal lumbar interbody fusion for degenerative lumbar spondylolisthesis].Zhongguo Gu Shang. 2023 May 25;36(5):414-9. doi: 10.12200/j.issn.1003-0034.2023.05.004. Zhongguo Gu Shang. 2023. PMID: 37211931 Chinese.
-
Comparison of Outcomes between Robot-Assisted Minimally Invasive Transforaminal Lumbar Interbody Fusion and Oblique Lumbar Interbody Fusion in Single-Level Lumbar Spondylolisthesis.Orthop Surg. 2021 Oct;13(7):2093-2101. doi: 10.1111/os.13151. Epub 2021 Oct 1. Orthop Surg. 2021. PMID: 34596342 Free PMC article.
-
Clinical and Radiographic Comparison of Oblique Lateral Lumbar Interbody Fusion and Minimally Invasive Transforaminal Lumbar Interbody Fusion in Patients with L4/5 grade-1 Degenerative Spondylolisthesis.Orthop Surg. 2023 Jun;15(6):1477-1487. doi: 10.1111/os.13360. Epub 2023 May 8. Orthop Surg. 2023. PMID: 37154089 Free PMC article.
-
Minimally invasive transforaminal lumbar interbody fusion versus oblique lateral interbody fusion for lumbar degenerative disease: a meta-analysis.BMC Musculoskelet Disord. 2021 Sep 18;22(1):802. doi: 10.1186/s12891-021-04687-7. BMC Musculoskelet Disord. 2021. PMID: 34537023 Free PMC article.
Cited by
-
Comparison of the Outcomes of Endoscopic Posterolateral Interbody Fusion and Lateral Interbody Fusion in the Treatment of Lumbar Degenerative Disease: A Systematic Review and Network Meta-Analysis.Orthop Surg. 2025 May;17(5):1287-1297. doi: 10.1111/os.14371. Epub 2025 Feb 3. Orthop Surg. 2025. PMID: 39895414 Free PMC article.
-
Meta-analysis of minimally invasive transforaminal lumbar interbody fusion versus oblique lumbar interbody fusion for treating lumbar degenerative diseases.J Orthop Surg Res. 2024 Dec 30;19(1):891. doi: 10.1186/s13018-024-05422-3. J Orthop Surg Res. 2024. PMID: 39736715 Free PMC article.
-
Full-endoscopic posterior lumbar interbody fusion for the treatment of lumbar degenerative diseases: a technical note with 2-year follow-up.J Orthop Surg Res. 2025 Mar 15;20(1):286. doi: 10.1186/s13018-025-05632-3. J Orthop Surg Res. 2025. PMID: 40087787 Free PMC article.
-
Feasibility of Ipsilateral Revision Oblique Lateral Interbody Fusion for Adjacent Segment Disease After Primary Oblique Lateral Interbody Fusion: A Retrospective Case Series.Cureus. 2025 Jul 15;17(7):e87961. doi: 10.7759/cureus.87961. eCollection 2025 Jul. Cureus. 2025. PMID: 40821200 Free PMC article.
References
-
- Foley KT, Lefkowitz MA. Advances in minimally invasive spine surgery. Clin. Neurosurg. 2002;49:499–517. - PubMed
-
- Foley, K. T., Holly, L. T., Schwender, J. D. Minimally invasive lumbar fusion. Spine (Phila Pa 1976). 2003; 28(15 Suppl): 26–35. - PubMed
-
- Bin Abd Razak HR, Dhoke P, Tay KS, et al. Single-level minimally invasive transforaminal lumbar interbody fusion provides sustained improvements in clinical and radiological outcomes up to 5 years postoperatively in patients with neurogenic symptoms secondary to spondylolisthesis. Asian Spine J. 2017;11:204–212. doi: 10.4184/asj.2017.11.2.204. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
