

Health care utilization and the associated costs attributable to cardiovascular disease in Ireland: a cross-sectional study
- PMID: 38383606
- PMCID: PMC11736149
- DOI: 10.1093/ehjqcco/qcae014
Health care utilization and the associated costs attributable to cardiovascular disease in Ireland: a cross-sectional study
Abstract
Background: Cardiovascular disease (CVD) is the leading cause of mortality and disability globally. We examined healthcare service utilization and costs attributable to CVD in Ireland in the period before the introduction of a major healthcare reform in 2016.
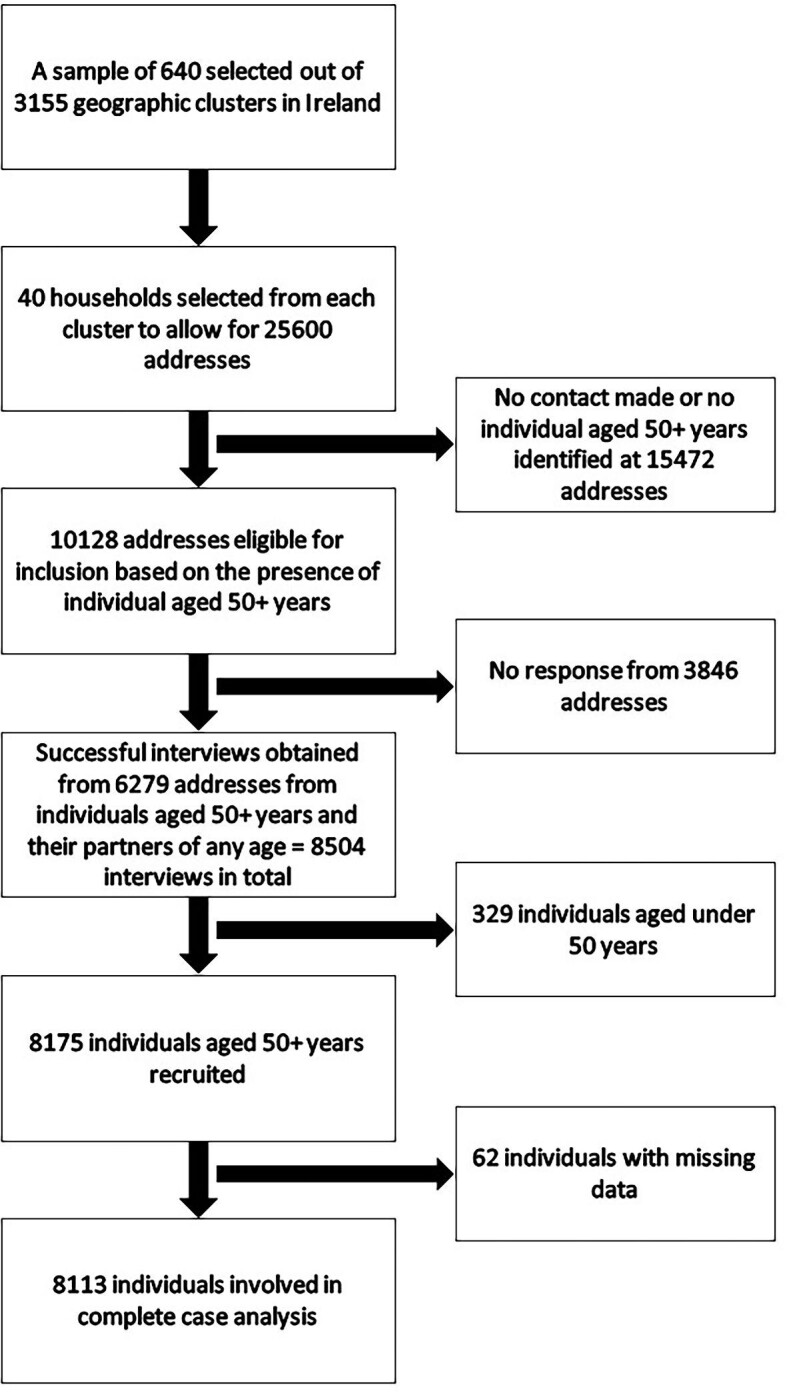
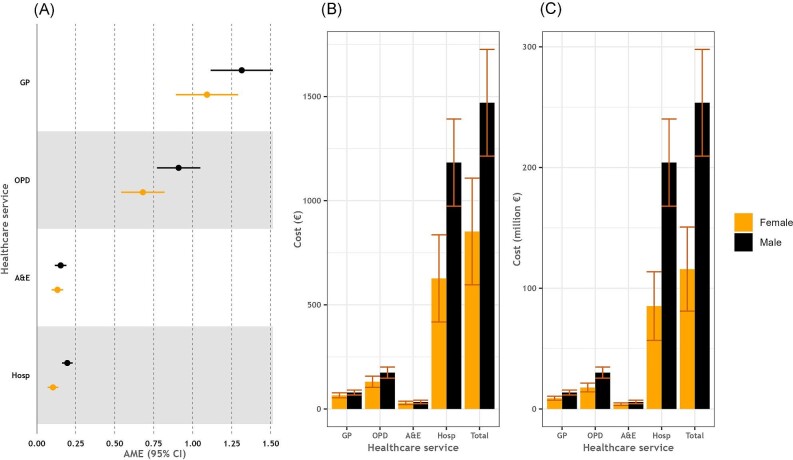
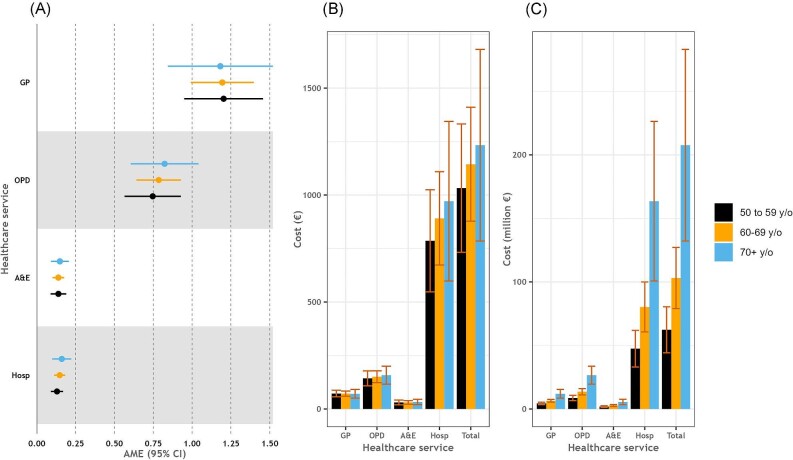
Methods: Secondary analysis of data from 8113 participants of the first wave of The Irish Longitudinal Study on Ageing. Cardiovascular disease was defined as having a self-reported doctor's diagnosis of myocardial infarction, angina, heart failure, stroke, atrial fibrillation, or transient ischaemic attack. Participants self-reported the utilization of healthcare services in the year preceding the interview. Negative binomial regression with average marginal effects (AMEs) was used to estimate the incremental number of general practitioner (GP) and outpatient department (OPD) visits, accident and emergency department attendances and hospitalizations in population with CVD relative to population without CVD. We calculated the corresponding costs at individual and population levels, by gender and age groups.
Results: The prevalence of CVD was 18.2% (95% CI: 17.3, 19.0) Participants with CVD reported higher utilization of all healthcare services. In adjusted models, having CVD was associated with incremental 1.19 [95% confidence interval (CI): 0.99, 1.39] GP and 0.79 (95% CI: 0.65, 0.93) OPD visits. There were twice as many incremental hospitalizations in males with CVD compared to females with CVD [AME (95% CI): 0.20 (0.16, 0.23) vs. 0.10 (0.07, 0.14)]. The incremental cost of healthcare service use in population with CVD was an estimated €352.2 million (95% CI: €272.8, €431.7), 93% of which was due to use of secondary care services.
Conclusion: We identified substantially increased use of healthcare services attributable to CVD in Ireland. Continued efforts aimed at CVD primary prevention and management are required.
Keywords: Cardiovascular disease; Direct costs; Healthcare use; Ireland.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Similar articles
-
Health service utilization and related costs attributable to diabetes.Diabet Med. 2018 Dec;35(12):1727-1734. doi: 10.1111/dme.13806. Epub 2018 Sep 19. Diabet Med. 2018. PMID: 30153351
-
Differences in All-Cause Health Care Utilization and Costs in a Type 2 Diabetes Mellitus Population with and Without a History of Cardiovascular Disease.J Manag Care Spec Pharm. 2018 Mar;24(3):280-290. doi: 10.18553/jmcp.2018.24.3.280. J Manag Care Spec Pharm. 2018. PMID: 29485954 Free PMC article.
-
Longitudinal Medication Adherence in Older Adults With Multimorbidity and Association With Health Care Utilization: Results From the Irish Longitudinal Study on Ageing.Ann Pharmacother. 2021 Jan;55(1):5-14. doi: 10.1177/1060028020937996. Epub 2020 Jul 1. Ann Pharmacother. 2021. PMID: 32608252
-
Projected Costs of Informal Caregiving for Cardiovascular Disease: 2015 to 2035: A Policy Statement From the American Heart Association.Circulation. 2018 May 8;137(19):e558-e577. doi: 10.1161/CIR.0000000000000570. Epub 2018 Apr 9. Circulation. 2018. PMID: 29632217 Review.
-
Cardiovascular Disease Healthcare Utilization in Sub-Saharan Africa: A Scoping Review.Int J Environ Res Public Health. 2019 Feb 1;16(3):419. doi: 10.3390/ijerph16030419. Int J Environ Res Public Health. 2019. PMID: 30717120 Free PMC article.
Cited by
-
Optimisation of Remote Monitoring Programmes in Heart Failure: Evaluation of Patient Drop-Out Behaviour and Healthcare Professionals' Perspectives.Healthcare (Basel). 2024 Jun 26;12(13):1271. doi: 10.3390/healthcare12131271. Healthcare (Basel). 2024. PMID: 38998806 Free PMC article.
-
Goal attainment, medication adherence and guideline adherence in the treatment of hypertension and dyslipidemia in Irish populations: A systematic review and meta-analysis.Int J Cardiol Cardiovasc Risk Prev. 2025 Jan 4;24:200364. doi: 10.1016/j.ijcrp.2025.200364. eCollection 2025 Mar. Int J Cardiol Cardiovasc Risk Prev. 2025. PMID: 39877073 Free PMC article. Review.
-
The effect of sociodemographic, socioeconomic, and health factors on healthcare utilization in cardiovascular patients in Serbia: a part of National Health Survey.Front Public Health. 2025 Jul 17;13:1569741. doi: 10.3389/fpubh.2025.1569741. eCollection 2025. Front Public Health. 2025. PMID: 40746687 Free PMC article.
References
-
- Ritchie H, Spooner F, Roser M. Causes of death Our World in Data 2018; Available from: https://ourworldindata.org/causes-of-death.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
