

Evaluation of Survival Outcomes Among Black and White Patients with Metastatic Castration-resistant Prostate Cancer: A Systematic Review and Meta-analysis
- PMID: 38384441
- PMCID: PMC10879936
- DOI: 10.1016/j.euros.2024.01.004
Evaluation of Survival Outcomes Among Black and White Patients with Metastatic Castration-resistant Prostate Cancer: A Systematic Review and Meta-analysis
Abstract
Context: Data on racial disparities among patients with metastatic castration-resistant prostate cancer (mCRPC) are limited and there is no uniform conclusion on differences by race in this setting.
Objective: To provide the latest evidence on racial disparities in survival outcomes between Black and White patients receiving systemic therapies for mCRPC.
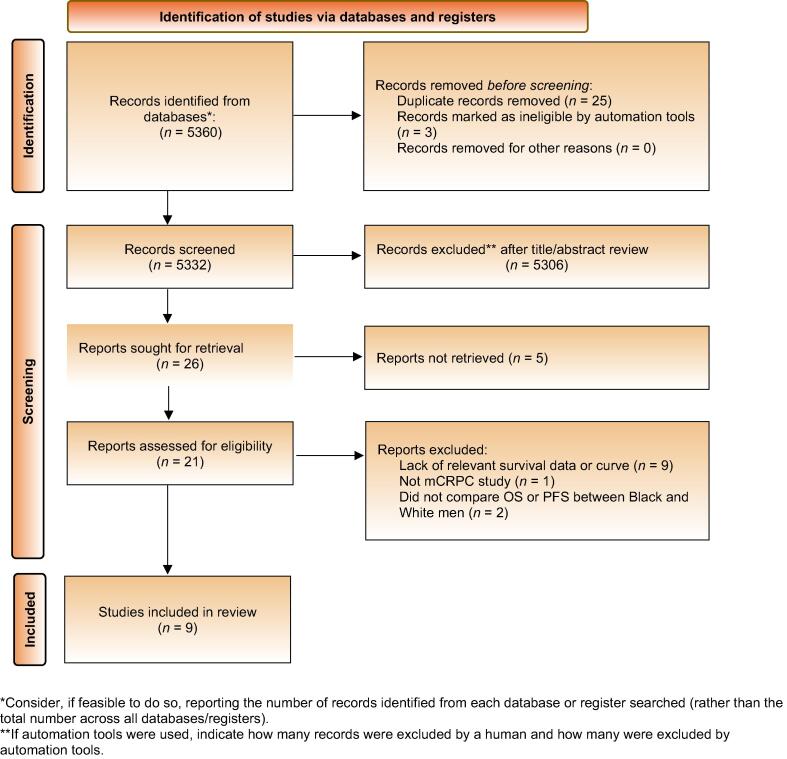
Evidence acquisition: Our study was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. We systematically searched the PubMed, Web of Science, and Cochrane Library databases up to September 2023 to identify potentially relevant studies. Overall survival (OS) and progression-free survival (PFS) were the outcomes of interest. Pooled hazard ratios (HRs) with 95% confidence intervals (CIs) were evaluated.
Evidence synthesis: Nine studies involving 9462 patients with mCRPC (2058 Black and 7404 White men) met the eligibility criteria and were included. Pooled estimates demonstrated significantly better OS for Black than for White men (HR 0.75, 95% CI 0.70-0.80; p < 0.0001). The results were similar in a subgroup of men receiving androgen receptor-targeted therapies (HR 0.72, 95% CI 0.66-0.78; p < 0.0001) and a subgroup of men receiving other treatments (HR 0.79, 95% CI 0.71-0.88; p < 0.0001). Likewise, significantly favorable PFS was observed for Black men receiving ARTs in comparison to their White counterparts (HR 0.84, 95% CI 0.71-0.99; p = 0.0373).
Conclusions: Overall, our meta-analysis of survival outcomes for men with mCRPC stratified by race revealed a significant survival benefit for Black men in comparison to their White counterparts, regardless of systemic therapeutic agent.
Patient summary: Both biological and nonbiological factors could account for racial differences in the efficacy of systemic treatments for metastatic prostate cancer that is resistant to hormone therapy. Our review provides the latest reliable evidence showing better survival outcomes for Black than for White men. The results will be helpful in further understanding the molecular mechanisms that might explain racial differences in this disease stage and in planning treatment.
Keywords: African American; Efficacy; Hormone therapy; Metastatic castration-resistant prostate cancer; Race.
© 2024 The Authors.
Figures


Similar articles
-
Individual Patient Data Analysis of Randomized Clinical Trials: Impact of Black Race on Castration-resistant Prostate Cancer Outcomes.Eur Urol Focus. 2016 Dec;2(5):532-539. doi: 10.1016/j.euf.2016.03.010. Epub 2016 Apr 1. Eur Urol Focus. 2016. PMID: 28723519
-
Outcomes Among African American and Non-Hispanic White Men With Metastatic Castration-Resistant Prostate Cancer With First-Line Abiraterone.JAMA Netw Open. 2022 Jan 4;5(1):e2142093. doi: 10.1001/jamanetworkopen.2021.42093. JAMA Netw Open. 2022. PMID: 34985518 Free PMC article.
-
Prognostic Value of Androgen Receptor Splice Variant 7 in the Treatment of Metastatic Castration-Resistant Prostate Cancer: A Systematic Review and Meta-Analysis.Front Oncol. 2020 Nov 30;10:562504. doi: 10.3389/fonc.2020.562504. eCollection 2020. Front Oncol. 2020. PMID: 33330031 Free PMC article.
-
Survival of Patients with Metastatic Prostate Cancer After Disease Progression on an Androgen Receptor Axis-Targeted Therapy Given in the Metastatic Castration-Sensitive Versus Metastatic Castration-Resistant Prostate Cancer Setting.Eur Urol Focus. 2023 Jan;9(1):106-109. doi: 10.1016/j.euf.2022.06.015. Epub 2022 Jul 11. Eur Urol Focus. 2023. PMID: 35835693
-
[177Lu]Lu-PSMA-Radioligand Therapy Efficacy Outcomes in Taxane-Naïve Versus Taxane-Treated Patients with Metastatic Castration-Resistant Prostate Cancer: A Systematic Review and Metaanalysis.J Nucl Med. 2023 Aug;64(8):1266-1271. doi: 10.2967/jnumed.123.265414. Epub 2023 May 11. J Nucl Med. 2023. PMID: 37169534
Cited by
-
Prostate Cancer Among Black Men in Canada.JAMA Netw Open. 2024 Jun 3;7(6):e2418475. doi: 10.1001/jamanetworkopen.2024.18475. JAMA Netw Open. 2024. PMID: 38916889 Free PMC article.
-
The association between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) and risk of prostate cancer: a retrospective study.PeerJ. 2025 Mar 14;13:e19065. doi: 10.7717/peerj.19065. eCollection 2025. PeerJ. 2025. PMID: 40098813 Free PMC article.
References
-
- Farkas A., Marcella S., Rhoads G.G. Ethnic and racial differences in prostate cancer incidence and mortality. Ethnicity Dis. 2000;10:69–75. - PubMed
-
- Nyame Y.A., Cooperberg M.R., Cumberbatch M.G., et al. Deconstructing, addressing, and eliminating racial and ethnic inequities in prostate cancer care. Eur Urol. 2022;82:341–351. - PubMed
-
- Arenas-Gallo C., Owiredu J., Weinstein I., et al. Race and prostate cancer: genomic landscape. Nat Rev Urol. 2022;19:547–561. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
