

A novel nomogram to predict the overall survival of early-stage hepatocellular carcinoma patients following ablation therapy
- PMID: 38384805
- PMCID: PMC10880021
- DOI: 10.3389/fonc.2024.1340286
A novel nomogram to predict the overall survival of early-stage hepatocellular carcinoma patients following ablation therapy
Abstract
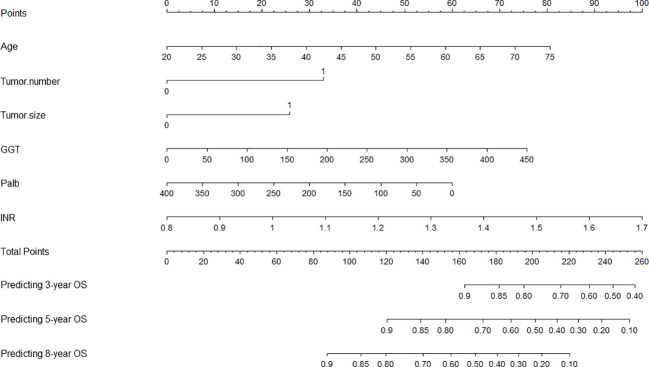
Introduction: This study aimed to assess factors affecting the prognosis of early-stage hepatocellular carcinoma (HCC) patients undergoing ablation therapy and create a nomogram for predicting their 3-, 5-, and 8-year overall survival (OS).
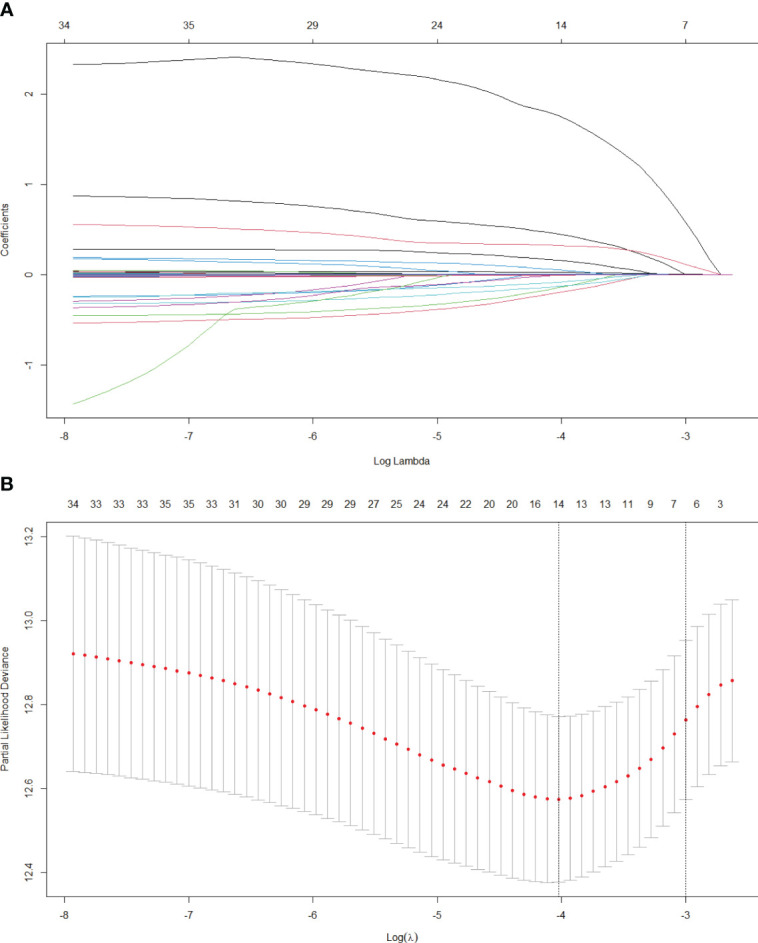
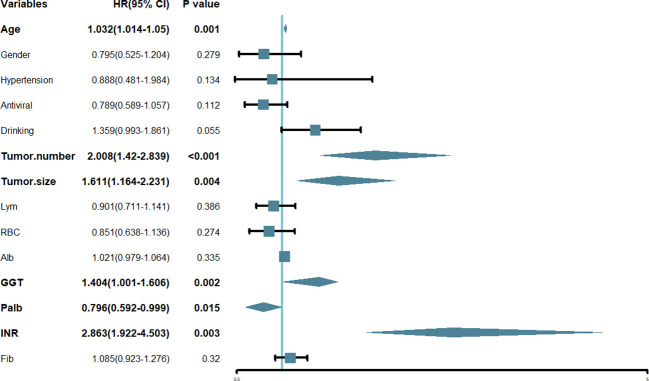
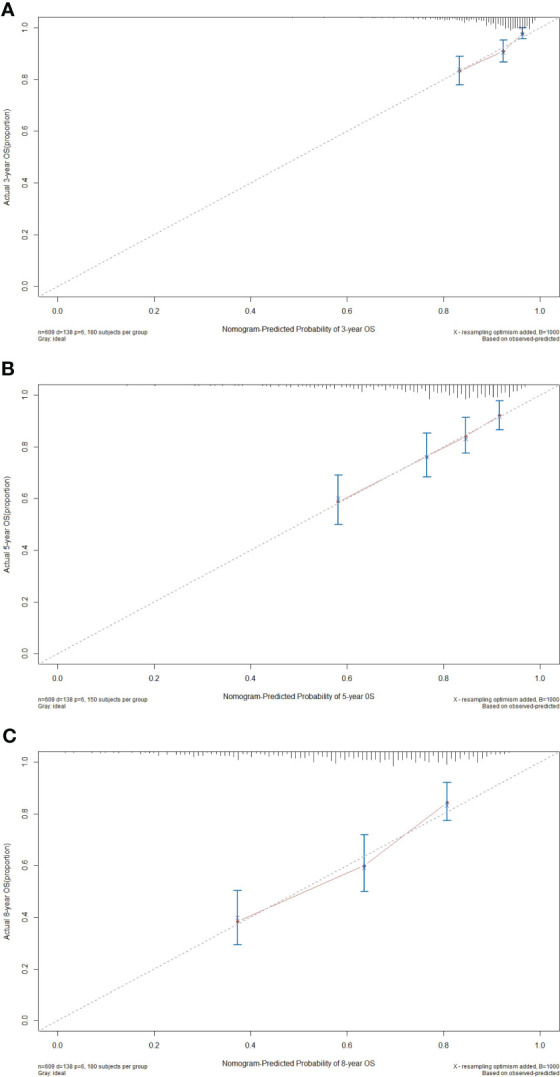
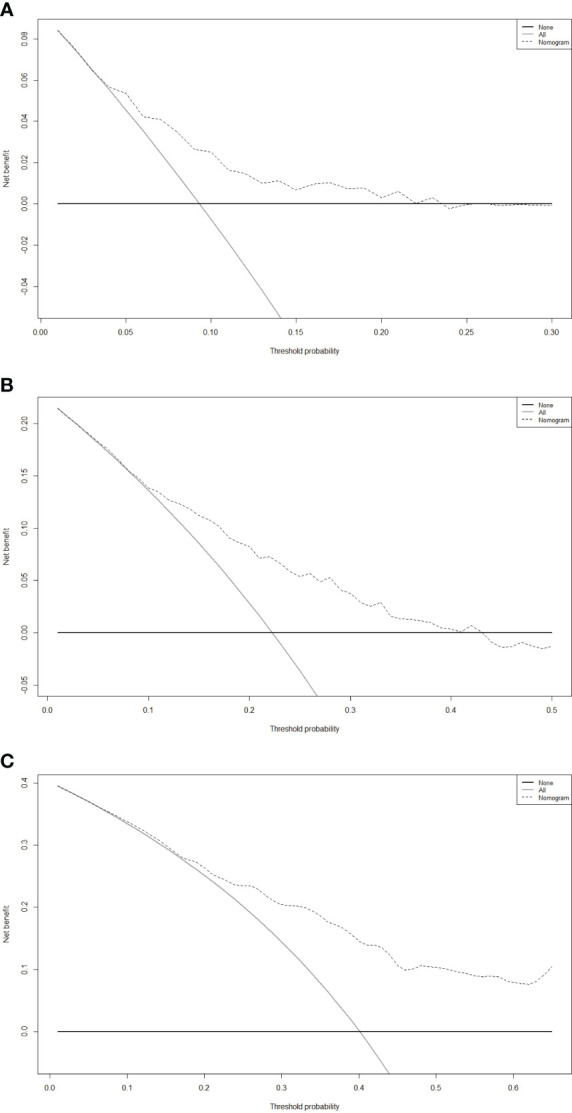
Methods: The research included 881 early-stage HCC patients treated at Beijing You'an Hospital, affiliated with Capital Medical University, from 2014 to 2022. A nomogram was developed using independent prognostic factors identified by Lasso and multivariate Cox regression analyses. Its predictive performance was evaluated with concordance index (C-index), receiver operating characteristic curve (ROC), calibration curve, and decision curve analysis (DCA).
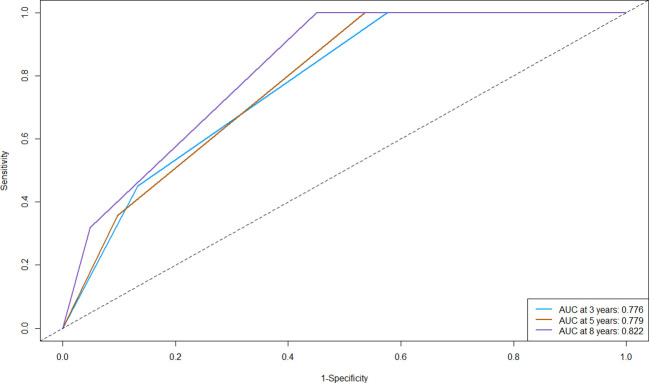
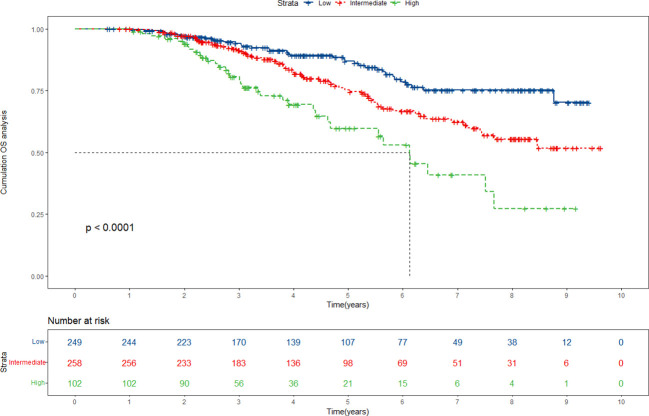
Results: The study identified age, tumor number, tumor size, gamma-glutamyl transpeptidase (GGT), international normalized ratio (INR), and prealbumin (Palb) as independent prognostic risk factors. The nomogram achieved C-indices of 0.683 (primary cohort) and 0.652 (validation cohort), with Area Under the Curve (AUC) values of 0.776, 0.779, and 0.822 (3-year, 5-year, and 8-year OS, primary cohort) and 0.658, 0.724, and 0.792 (validation cohort), indicating that the nomogram possessed strong discriminative ability. Calibration and DCA curves further confirmed the nomogram's predictive accuracy and clinical utility. The nomogram can effectively stratify patients into low-, intermediate-, and high-risk groups, particularly identifying high-risk patients.
Conclusions: The established nomogram in our study can provide precise prognostic information for HCC patients following ablation treatment and enable physicians to accurately identify high-risk individuals and facilitate timely intervention.
Keywords: Lasso regression; ablation; hepatocellular carcinoma; multivariate Cox regression; nomogram; overall survival.
Copyright © 2024 Zhang, Sheng, Qiao, Han and Jin.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Prognostic nomogram based on the gamma-glutamyl transpeptidase-to-platelet ratio for patients with compensated cirrhotic hepatocellular carcinoma after local ablation.Front Oncol. 2024 Jul 11;14:1406764. doi: 10.3389/fonc.2024.1406764. eCollection 2024. Front Oncol. 2024. PMID: 39055565 Free PMC article.
-
Prognostic model for predicting recurrence in hepatocellular carcinoma patients with high systemic immune-inflammation index based on machine learning in a multicenter study.Front Immunol. 2024 Sep 9;15:1459740. doi: 10.3389/fimmu.2024.1459740. eCollection 2024. Front Immunol. 2024. PMID: 39315112 Free PMC article.
-
Nomogram built based on machine learning to predict recurrence in early-stage hepatocellular carcinoma patients treated with ablation.Front Oncol. 2024 May 10;14:1395329. doi: 10.3389/fonc.2024.1395329. eCollection 2024. Front Oncol. 2024. PMID: 38800405 Free PMC article.
-
Machine Learning-Based Nomogram for Predicting Overall Survival in Elderly Patients with Cirrhotic Hepatocellular Carcinoma Undergoing Ablation Therapy.J Hepatocell Carcinoma. 2024 Mar 7;11:509-523. doi: 10.2147/JHC.S450825. eCollection 2024. J Hepatocell Carcinoma. 2024. PMID: 38468611 Free PMC article.
-
Nomogram for predicting post-therapy recurrence in BCLC A/B hepatocellular carcinoma with Child-Pugh B cirrhosis.Front Immunol. 2024 May 10;15:1369988. doi: 10.3389/fimmu.2024.1369988. eCollection 2024. Front Immunol. 2024. PMID: 38799452 Free PMC article.
Cited by
-
Gamma-Glutamyl Transpeptidase to Neutrophil Ratio as Prognostic Indicator for Hepatocellular Carcinoma Patients Post-Curative Resection.J Hepatocell Carcinoma. 2024 Oct 27;11:2077-2085. doi: 10.2147/JHC.S478186. eCollection 2024. J Hepatocell Carcinoma. 2024. PMID: 39483455 Free PMC article.
-
A novel nomogram based on complement C3 to predict the overall survival of early-stage hepatocellular carcinoma patients with microvascular invasion-positive undergoing curative resection.Front Oncol. 2025 Feb 20;15:1559083. doi: 10.3389/fonc.2025.1559083. eCollection 2025. Front Oncol. 2025. PMID: 40052130 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous