

Relationship between extravascular leakage and clinical outcome on computed tomography of isolated traumatic brain injury
- PMID: 38385145
- PMCID: PMC10879720
- DOI: 10.1002/ams2.931
Relationship between extravascular leakage and clinical outcome on computed tomography of isolated traumatic brain injury
Abstract
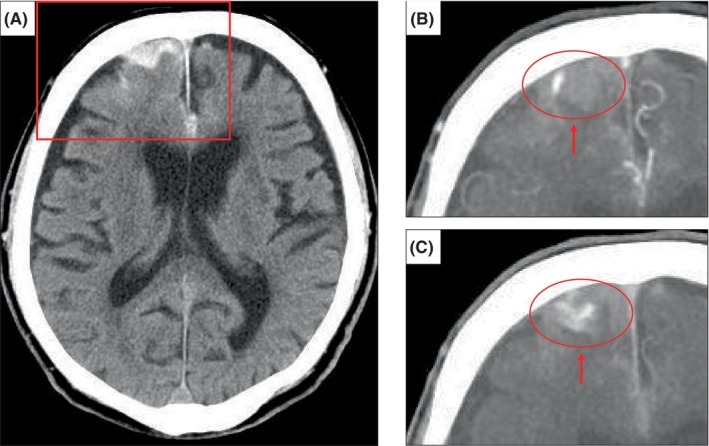
Aim: This study investigated whether contrast extravasation on computed tomography (CT) angiography in patients with traumatic brain injury (TBI) is associated with death or surgical procedures.
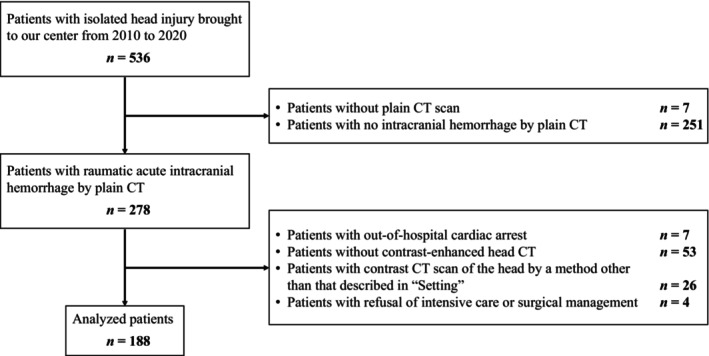
Methods: Patients over 18 years old, directly brought in by ambulance with an isolated head injury and confirmed to have acute intracranial hemorrhage on a CT scan upon admission between 2010 and 2020, were included. The primary outcome was mortality, and the secondary outcome was neurosurgical procedures performed from admission to discharge from the intensive care unit. Multivariable logistic regression analyses were performed to evaluate the association between these outcomes and contrast extravasation.
Results: The analysis included 188 patients with a median age of 65 years, 123 men (65.4%), 34 deaths (18.1%), and 91 surgeries (48.4%). Among the 66 patients with contrast extravasation, 22 (33.3%) died and 47 (71.2%) required surgery. Among the 122 patients with no contrast extravasation, 12 (9.8%) died, and 44 (36.1%) required surgery. The presence or absence of extravascular leakage was associated with death (odds ratio, 3.6 [95% CI: 1.2-12.2]) and surgery (odds ratio, 7.6 [95% CI: 2.5-22.7]).
Conclusion: Contrast extravasation was associated with mortality and performance of surgery in patients with an isolated head injury.
Keywords: contrast extravasation; head injury; mortality; surgery.
© 2024 The Authors. Acute Medicine & Surgery published by John Wiley & Sons Australia, Ltd on behalf of Japanese Association for Acute Medicine.
Conflict of interest statement
Dr. Hiroshi Ogura and Dr. Oda Jun are the Editorial Board members of AMS Journal and the co‐authors of this article. Dr. Jun Oda is the Editor‐in‐Chief of the journal. To minimize bias, they were excluded from all editorial decision‐making related to the acceptance of this article for publication. Peer review was handled independently by the AMS Journal editorial office and Dr. Yasuyuki Kuwagata as the Editor to minimize bias.
Figures

Similar articles
-
Association of Extravascular Leakage on Computed Tomography Angiography with Fibrinogen Levels at Admission in Patients with Traumatic Brain Injury.Neurotrauma Rep. 2022 Dec 26;4(1):3-13. doi: 10.1089/neur.2022.0054. eCollection 2022. Neurotrauma Rep. 2022. PMID: 36636245 Free PMC article.
-
Role of repeat CT in mild to moderate head injury: an institutional study.Neurosurg Focus. 2019 Nov 1;47(5):E2. doi: 10.3171/2019.8.FOCUS19527. Neurosurg Focus. 2019. PMID: 31675712
-
Contrast extravasation on computed tomography angiography predicts clinical outcome in primary intracerebral hemorrhage: a prospective study of 139 cases.Stroke. 2011 Dec;42(12):3441-6. doi: 10.1161/STROKEAHA.111.623405. Epub 2011 Oct 6. Stroke. 2011. PMID: 21980207
-
The extravasation of contrast as a predictor of cerebral hemorrhagic contusion expansion, poor neurological outcome and mortality after traumatic brain injury: A systematic review and meta-analysis.PLoS One. 2020 Jul 7;15(7):e0235561. doi: 10.1371/journal.pone.0235561. eCollection 2020. PLoS One. 2020. PMID: 32634141 Free PMC article.
-
[Value of serial CT scanning and intracranial pressure monitoring for detecting new intracranial mass effect in severe head injury patients showing lesions type I-II in the initial CT scan].Neurocirugia (Astur). 2005 Jun;16(3):217-34. Neurocirugia (Astur). 2005. PMID: 16007322 Review. Spanish.
References
-
- Eastman AL, Chason DP, Perez CL, McAnulty AL, Minei JP. Computed tomographic angiography for the diagnosis of blunt cervical vascular injury: is it ready for primetime? J Trauma. 2006;60:925–929. - PubMed
-
- Geeraerts T, Velly L, Abdennour L, Asehnoune K, Audibert G, Bouzat P, et al. Management of severe traumatic brain injury (first 24 hours). Anaesth Crit Care Pain Med. 2018;37:171–186. - PubMed
-
- Huang APH, Lee CW, Hsieh HJ, Yang CC, Tsai YH, Tsuang FY, et al. Early parenchymal contrast extravasation predicts subsequent hemorrhage progression, clinical deterioration, and need for surgery in patients with traumatic cerebral contusion. J Trauma. 2011;71:1593–1599. - PubMed
-
- Rosa M Jr, da Rocha AJ, Maia AC Jr, Saade N, Veiga JC, Romero JM. Contusion contrast extravasation depicted on multidetector computed tomography angiography predicts growth and mortality in traumatic brain contusion. J Neurotrauma. 2016;33:1015–1022. - PubMed
LinkOut - more resources
Full Text Sources
