

[Comparison of effectiveness between unilateral biportal endoscopic decompression and unilateral biportal endoscopic lumbar interbody fusion for degree Ⅰ degenerative lumbar spondylolisthesis]
- PMID: 38385229
- PMCID: PMC10882227
- DOI: 10.7507/1002-1892.202311025
[Comparison of effectiveness between unilateral biportal endoscopic decompression and unilateral biportal endoscopic lumbar interbody fusion for degree Ⅰ degenerative lumbar spondylolisthesis]
Abstract
Objective: To compare the effectiveness of unilateral biportal endoscopic decompression and unilateral biportal endoscopic lumbar interbody fusion (ULIF) in the treatment of degreeⅠdegenerative lumbar spondylolisthesis (DLS).
Methods: A clinical data of 58 patients with degreeⅠDLS who met the selection criteria between October 2021 and October 2022 was retrospectively analyzed. Among them, 28 cases were treated with unilateral biportal endoscopic decompression (decompression group) and 30 cases with ULIF (ULIF group). There was no significant difference between the two groups ( P>0.05) in the gender, age, lesion segment, and preoperative visual analogue scale (VAS) score of low back pain, VAS score of leg pain, Oswestry disability index (ODI), C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), disk height (DH), segmental lordosis (SL), and other baseline data. The operation time, postoperative drainage volume, postoperative ambulation time, VAS score of low back pain, VAS score of leg pain, ODI, laboratory examination indexes (CRP, ESR), and imaging parameters (DH, SL) were compared between the two groups.
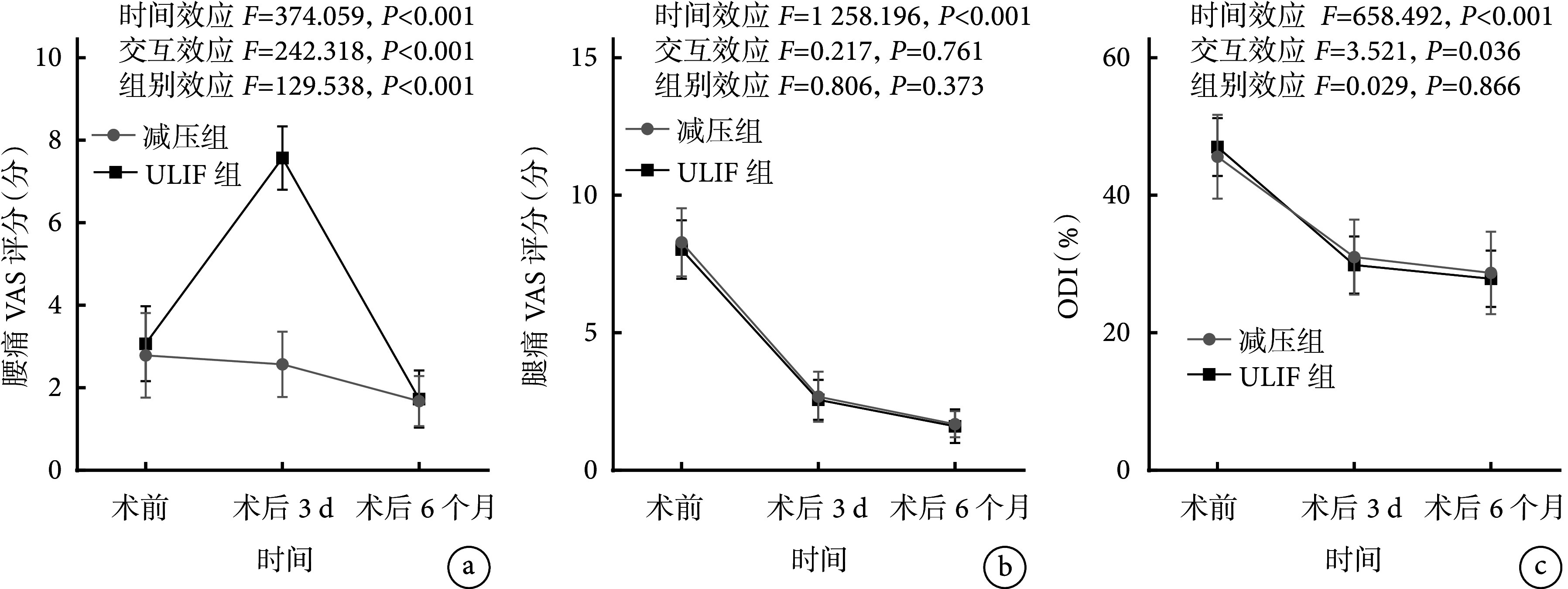
Results: Compared with the ULIF group, the decompression group had shorter operation time, less postoperative drainage, and earlier ambulation ( P<0.05). All incisions healed by first intention, and no complication such as nerve root injury, epidural hematoma, or infection occurred. All patients were followed up 12 months. Laboratory tests showed that ESR and CRP at 3 days after operation in decompression group were not significantly different from those before operation ( P>0.05), while the above indexes in ULIF group significantly increased at 3 days after operation compared to preoperative values ( P<0.05). There were significant differences in the changes of ESR and CRP before and after operation between the two groups ( P<0.05). Except that the VAS score of low back pain at 3 days after operation was not significantly different from that before operation in decompression group ( P>0.05), there were significant differences in VAS score of low back pain and VAS score of leg pain between the two groups at other time points ( P<0.05). The VAS score of low back pain in ULIF group was significantly higher than that in decompression group at 3 days after operation ( P<0.05), and there was no significant difference in VAS score of low back pain and VAS score of leg pain between the two groups at other time points ( P>0.05). The ODI of the two groups significantly improved after operation ( P<0.05), but there was no significant difference between 3 days and 6 months after operation ( P>0.05). There was no significant difference between the two groups at the two time points after operation ( P<0.05). Imaging examination showed that there was no significant difference in DH and SL between pre-operation and 12 months after operation in decompression group ( P>0.05). However, the above two indexes in ULIF group were significantly higher than those before operation ( P<0.05). There were significant differences in the changes of DH and SL before and after operation between the two groups ( P<0.05).
Conclusion: Unilateral biportal endoscopic decompression can achieve good effectiveness in the treatment of degree Ⅰ DLS. Compared with ULIF, it can shorten operation time, reduce postoperative drainage volume, promote early ambulation, reduce inflammatory reaction, and accelerate postoperative recovery. ULIF has more advantages in restoring intervertebral DH and SL.
目的: 比较单侧双通道内镜(unilateral biportal endoscopy,UBE)下单纯减压与腰椎椎间融合术(unilateral biportal endoscopic lumbar interbody fusion,ULIF)治疗Ⅰ度退变性腰椎滑脱(degenerative lumbar spondylolisthesis,DLS)的疗效。.
方法: 回顾性分析2021年10月—2022年10月收治并符合选择标准的58例Ⅰ度DLS患者临床资料,其中采用UBE下单纯减压治疗28例(减压组)、ULIF治疗30例(ULIF组)。两组患者性别、年龄、手术节段以及术前腰痛疼痛视觉模拟评分(VAS)、腿痛VAS评分、Oswestry 功能障碍指数(ODI)、C反应蛋白(C-reactive protein,CRP)、红细胞沉降率 (erythrocyte sedimentation rate,ESR)、椎间盘高度(disk height,DH)、节段前凸(segmental lordosis,SL)等基线资料比较,差异均无统计学意义( P>0.05)。比较两组手术时间、术后引流量、术后离床活动时间,术后腰痛 VAS 评分、腿痛 VAS 评分、ODI、实验室检查指标(CRP、ESR)、影像学参数(DH、SL)。.
结果: 与ULIF 组相比,减压组手术时间短、术后引流量少且患者开始离床活动更早,差异均有统计学意义( P<0.05)。两组切口均Ⅰ期愈合,无神经根损伤、硬膜外血肿、感染等并发症发生。两组患者术后均获随访12个月。实验室检查示,减压组术后3 d ESR、CRP与术前差异均无统计学意义( P>0.05),而ULIF组术后3 d上述指标均较术前升高( P<0.05);两组间ESR、CRP手术前后差值比较,差异有统计学意义( P<0.05)。除减压组术后3 d腰痛VAS评分与术前差异无统计学意义( P>0.05)外,两组腰、腿痛VAS评分其他时间点间比较,差异均有统计学意义( P<0.05)。术后3 d ULIF组腰痛VAS评分高于减压组( P<0.05),其余时间点两组腰、腿痛VAS评分差异均无统计学意义( P>0.05)。两组术后ODI均较术前改善( P<0.05),但术后3 d与6个月间差异无统计学意义( P>0.05);术后两时间点组间差异均无统计学意义( P<0.05)。影像学检查示,减压组术后12个月DH、SL与术前差异无统计学意义( P>0.05);而ULIF组上述两指标均较术前升高,差异有统计学意义( P<0.05)。两组间DH、SL手术前后差值比较,差异有统计学意义( P<0.05)。.
结论: UBE下单纯减压治疗Ⅰ度DLS可取得良好疗效,与ULIF相比可缩短手术时间、减少术后引流量、促进患者早期离床活动,炎症反应小,术后恢复快;但ULIF对于恢复椎间盘高度、节段前凸更有优势。.
Keywords: Degenerative lumbar spondylolisthesis; decompression; lumbar interbody fusion; unilateral biportal endoscopy.
Conflict of interest statement
利益冲突 在课题研究和文章撰写过程中不存在利益冲突
Figures

Similar articles
-
[Comparison of effectiveness between unilateral biportal endoscopic lumbar interbody fusion and endoscopic transforaminal lumbar interbody fusion for lumbar spinal stenosis combined with intervertebral disc herniation].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2023 Sep 15;37(9):1098-1105. doi: 10.7507/1002-1892.202303095. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2023. PMID: 37718422 Free PMC article. Chinese.
-
[Prospective comparative study of unilateral biportal endoscopic transforaminal lumbar interbody fusion and endoscopic transforaminal lumbar interbody fusion for treatment of single-segment degenerative lumbar spinal stenosis with lumbar spondylolisthesis].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024 May 15;38(5):521-528. doi: 10.7507/1002-1892.202402058. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024. PMID: 38752236 Free PMC article. Clinical Trial. Chinese.
-
Oblique lateral interbody fusion (OLIF) compared with unilateral biportal endoscopic lumbar interbody fusion (ULIF) for degenerative lumbar spondylolisthesis: a 2-year follow-up study.J Orthop Surg Res. 2023 Aug 24;18(1):621. doi: 10.1186/s13018-023-04111-x. J Orthop Surg Res. 2023. PMID: 37620977 Free PMC article.
-
Unilateral biportal endoscopic lumbar interbody fusion versus minimally invasive transforaminal lumbar interbody fusion for single-segment lumbar degenerative disease: a meta-analysis.BMC Musculoskelet Disord. 2024 Nov 21;25(1):938. doi: 10.1186/s12891-024-08046-0. BMC Musculoskelet Disord. 2024. PMID: 39574056 Free PMC article.
-
Comparison of efficacy between unilateral biportal endoscopic lumbar fusion versus minimally invasive transforaminal lumbar fusion in the treatment of lumbar degenerative diseases: A systematic review and meta-analysis.Medicine (Baltimore). 2023 Aug 25;102(34):e34705. doi: 10.1097/MD.0000000000034705. Medicine (Baltimore). 2023. PMID: 37653732 Free PMC article.
References
-
- Shukla GG, Chilakapati SS, Matur AV, et al Laminectomy with fusion is associated with greater functional improvement compared with laminectomy alone for the treatment of degenerative lumbar spondylolisthesis: a systematic review and meta-analysis. Spine (Phila Pa 1976) 2023;48(12):874–884. doi: 10.1097/BRS.0000000000004673. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous