

Sympathetic Neural Control at Rest and During the Cold Pressor Test in Patients With Heart Failure With Preserved Ejection Fraction
- PMID: 38385250
- PMCID: PMC10954398
- DOI: 10.1161/HYPERTENSIONAHA.123.21918
Sympathetic Neural Control at Rest and During the Cold Pressor Test in Patients With Heart Failure With Preserved Ejection Fraction
Abstract
Background: We tested the hypothesis that patients with heart failure with preserved ejection fraction (HFpEF) would have greater muscle sympathetic nerve activity (MSNA) at rest and sympathetic reactivity during a cold pressor test compared with non-heart failure controls. Further, given the importance of the baroreflex modulation of MSNA in the control of blood pressure (BP), we hypothesized that patients with HFpEF would exhibit a reduced sympathetic baroreflex sensitivity.
Methods: Twenty-eight patients with HFpEF and 44 matched controls (mean±SD: 71±8 versus 70±7 years; 9 men/19 women versus 16 men/28 women) were studied. BP, heart rate, and MSNA (microneurography) were measured during 6 to 10 minutes of supine rest and the 2-minute cold pressor test. Spontaneous sympathetic baroreflex sensitivity was assessed during supine rest.
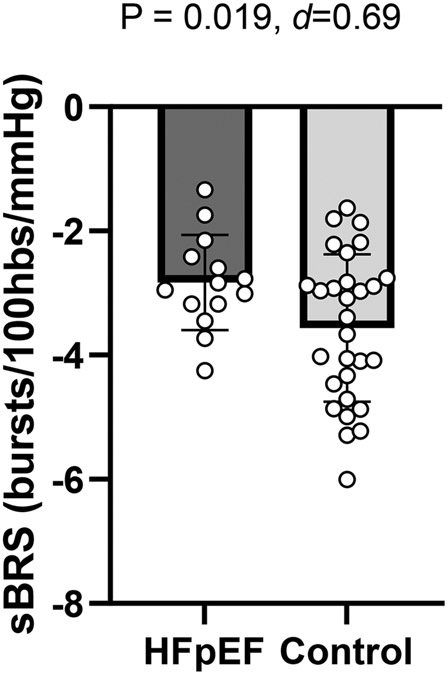
Results: Patients with HFpEF had higher resting MSNA burst frequency (39±14 versus 31±12 bursts/min; P=0.020) and lower sympathetic baroreflex sensitivity (-2.83±0.76 versus -3.57±1.19 bursts/100 heartbeats/mm Hg; P=0.019) than controls, but burst incidence was not different between groups (56±19 versus 50±20 bursts/100 heartbeats; P=0.179). During the cold pressor test, increases in MSNA indices did not differ between groups (P=0.135-0.998), but patients had a smaller increase in diastolic BP (Δ4±6 versus Δ14±11 mm Hg; P<0.001) compared with controls.
Conclusions: Despite augmented resting MSNA burst frequency, burst incidence was not significantly different between groups, and sympathetic baroreflex sensitivity was reduced in patients with HFpEF. Furthermore, patients had preserved sympathetic reactivity but attenuated diastolic BP responses during the cold pressor test. These data suggest that, during physiological stress, sympathetic reactivity is intact, but the peripheral pathway for sympathetic vasoconstriction may be impaired in HFpEF.
Keywords: aged; baroreflex; heart failure; sympathetic nervous system.
Conflict of interest statement
None.
Figures



Similar articles
-
Maintained sympathetic reactivity but blunted pressor response to static handgrip exercise in heart failure with preserved ejection fraction.Clin Auton Res. 2025 Jun;35(3):487-500. doi: 10.1007/s10286-025-01114-y. Epub 2025 Feb 26. Clin Auton Res. 2025. PMID: 40000578 Free PMC article.
-
The sympathetic nervous system in heart failure with preserved ejection fraction.Heart Fail Rev. 2025 Jan;30(1):209-218. doi: 10.1007/s10741-024-10456-0. Epub 2024 Oct 23. Heart Fail Rev. 2025. PMID: 39438394 Free PMC article. Review.
-
Arterial baroreflex regulation of muscle sympathetic nerve activity at rest and during stress.J Physiol. 2019 Sep;597(18):4729-4741. doi: 10.1113/JP278376. Epub 2019 Aug 25. J Physiol. 2019. PMID: 31368530
-
Sympathetic Response to 1-Leg Cycling Exercise Predicts Exercise Capacity in Patients With Heart Failure With Preserved Ejection Fraction.Circ Heart Fail. 2025 Jan;18(1):e011962. doi: 10.1161/CIRCHEARTFAILURE.124.011962. Epub 2024 Dec 6. Circ Heart Fail. 2025. PMID: 39641163
-
Sympathetic transduction at rest and during cold pressor test in young healthy non-Hispanic Black and White women.Am J Physiol Regul Integr Comp Physiol. 2023 Dec 1;325(6):R682-R691. doi: 10.1152/ajpregu.00073.2023. Epub 2023 Oct 2. Am J Physiol Regul Integr Comp Physiol. 2023. PMID: 37781734 Free PMC article.
Cited by
-
Treating heart failure by targeting the vagus nerve.Heart Fail Rev. 2024 Nov;29(6):1201-1215. doi: 10.1007/s10741-024-10430-w. Epub 2024 Aug 9. Heart Fail Rev. 2024. PMID: 39117958 Free PMC article. Review.
-
Prognostic significance of cold pressor test myocardial perfusion imaging in patients with ischemia and nonobstructive coronary arteries.Quant Imaging Med Surg. 2025 Aug 1;15(8):6763-6775. doi: 10.21037/qims-2025-33. Epub 2025 Jul 30. Quant Imaging Med Surg. 2025. PMID: 40785860 Free PMC article.
-
Maintained sympathetic reactivity but blunted pressor response to static handgrip exercise in heart failure with preserved ejection fraction.Clin Auton Res. 2025 Jun;35(3):487-500. doi: 10.1007/s10286-025-01114-y. Epub 2025 Feb 26. Clin Auton Res. 2025. PMID: 40000578 Free PMC article.
-
The sympathetic nervous system in heart failure with preserved ejection fraction.Heart Fail Rev. 2025 Jan;30(1):209-218. doi: 10.1007/s10741-024-10456-0. Epub 2024 Oct 23. Heart Fail Rev. 2025. PMID: 39438394 Free PMC article. Review.
-
Glutaminolysis and α-ketoglutarate-stimulated KCa3.1 expression contribute to β-adrenoceptor activation-induced myocardial fibrosis in mice.Sci China Life Sci. 2025 Jul;68(7):2043-2057. doi: 10.1007/s11427-024-2811-x. Epub 2025 May 7. Sci China Life Sci. 2025. PMID: 40343579
References
-
- Badrov MB, Keir DA, Tomlinson G, Notarius CF, Millar PJ, Kimmerly DS, Shoemaker JK, Keys E, Floras JS. Normal and excessive muscle sympathetic nerve activity in heart failure: implications for future trials of therapeutic autonomic modulation. Eur J Heart Fail. 2023;25:201–210. doi: 10.1002/ejhf.2749 - DOI - PubMed
-
- Waagstein F, Bristow MR, Swedberg K, Camerini F, Fowler MB, Silver MA, Gilbert EM, Johnson MR, Goss FG, Hjalmarson A. Beneficial effects of metoprolol in idiopathic dilated cardiomyopathy. Metoprolol in Dilated Cardiomyopathy (MDC) Trial Study Group. Lancet. 1993;342:1441–1446. doi: 10.1016/0140-6736(93)92930-r - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
