

Different pain phenotypes are associated with anti-Caspr2 autoantibodies
- PMID: 38386048
- PMCID: PMC11055745
- DOI: 10.1007/s00415-024-12224-4
Different pain phenotypes are associated with anti-Caspr2 autoantibodies
Abstract
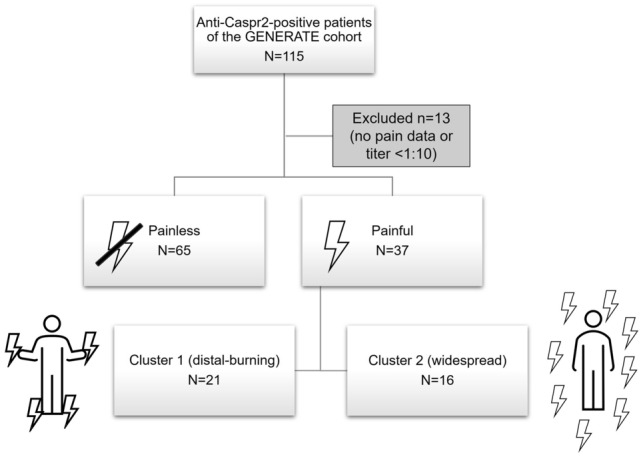
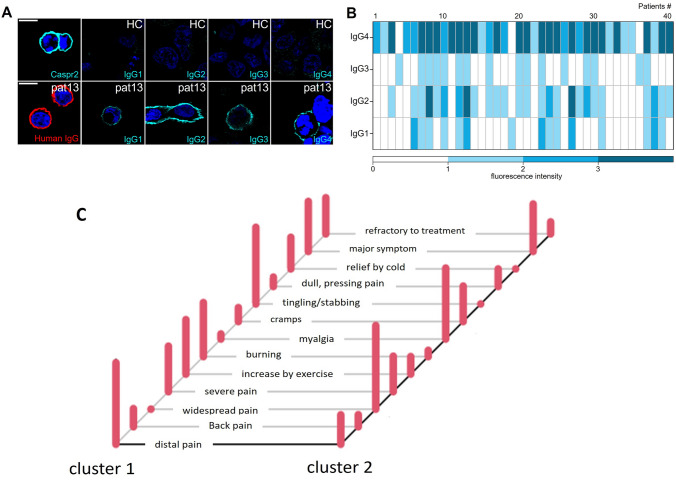
Autoantibodies against contactin-associated protein 2 (Caspr2) not only induce limbic autoimmune encephalitis but are also associated with pain conditions. Here, we analyzed clinical data on pain in a large cohort of patients included into the German Network for Research in Autoimmune Encephalitis. Out of 102 patients in our cohort, pain was a frequent symptom (36% of all patients), often severe (63.6% of the patients with pain) and/or even the major symptom (55.6% of the patients with pain). Pain phenotypes differed between patients. Cluster analysis revealed two major phenotypes including mostly distal-symmetric burning pain and widespread pain with myalgia and cramps. Almost all patients had IgG4 autoantibodies and some additional IgG1, 2, and/or 3 autoantibodies, but IgG subclasses, titers, and presence or absence of intrathecal synthesis were not associated with the occurrence of pain. However, certain pre-existing risk factors for chronic pain like diabetes mellitus, peripheral neuropathy, or preexisting chronic back pain tended to occur more frequently in patients with anti-Caspr2 autoantibodies and pain. Our data show that pain is a relevant symptom in patients with anti-Caspr2 autoantibodies and support the idea of decreased algesic thresholds leading to pain. Testing for anti-Caspr2 autoantibodies needs to be considered in patients with various pain phenotypes.
Keywords: Autoantibody; Caspr2; IgG subclass; IgG4; Pain.
© 2024. The Author(s).
Conflict of interest statement
This study was funded by the German Research Foundation, Clinical Research Group “ResolvePain” (KFO5001). CG received speaker and consultancy fees or travel compensation from Alexion, Sobi, Argenx. His research including the submitted work is funded by the German Federal Ministry of Education and Research (BMBF) through a grant for the Forschungsverbund CONNECT-GENERATE, grant code 01GM2208E, and outside the submitted work by the German Research Foundation and the Schilling foundation. JL received speaker fees or travel compensation from Roche, Teva, the Movement Disorders Society and the Cure Huntington’s Disease Initiative (CHDI). His institution has been reimbursed for his role as principal investigator in trials for SOM Biotech and CHDI. His research including the submitted work is funded by the German Federal Ministry of Education and Research (BMBF) through a grant for the Forschungsverbund CONNECT-GENERATE, grant code 01GM2208B, and outside the submitted work by the European Huntington’s Disease Network (EHDN) and Ministry for Education and Research Baden-Württemberg. FvP reports personal fees and grants from Bial, Desitin Arzneimittel, Eisai, GW Pharmaceutical companies, Arvelle Therapeutics, Zogenix, and UCB Pharma. HR received consultancy fees from Orion and Gruenenthal.
Figures
References
-
- Govert F, Abrante L, Becktepe J, Balint B, Ganos C, Hofstadt-van Oy U, Krogias C, Varley J, Irani SR, Paneva S, Titulaer MJ, de Vries JM, Boon AJW, Schreurs MWJ, Joubert B, Honnorat J, Vogrig A, Arino H, Sabater L, Dalmau J, Scotton S, Jacob S, Melzer N, Bien CG, Geis C, Lewerenz J, Pruss H, Wandinger KP, Deuschl G, Leypoldt F. Distinct movement disorders in contactin-associated-protein-like-2 antibody-associated autoimmune encephalitis. Brain. 2023;146:657–667. doi: 10.1093/brain/awac276. - DOI - PubMed
-
- van Sonderen A, Arino H, Petit-Pedrol M, Leypoldt F, Kortvelyessy P, Wandinger KP, Lancaster E, Wirtz PW, Schreurs MW, Sillevis Smitt PA, Graus F, Dalmau J, Titulaer MJ. The clinical spectrum of Caspr2 antibody-associated disease. Neurology. 2016;87:521–528. doi: 10.1212/WNL.0000000000002917. - DOI - PMC - PubMed
-
- Benoit J, Muniz-Castrillo S, Vogrig A, Farina A, Pinto AL, Picard G, Rogemond V, Guery D, Alentorn A, Psimaras D, Rheims S, Honnorat J, Joubert B. Early-stage contactin-associated protein-like 2 limbic encephalitis: clues for diagnosis. Neurology(R) Neuroimmunol Neuroinflamm. 2023 doi: 10.1212/NXI.0000000000200041. - DOI - PMC - PubMed
-
- Poliak S, Gollan L, Martinez R, Custer A, Einheber S, Salzer JL, Trimmer JS, Shrager P, Peles E. Caspr2, a new member of the neurexin superfamily, is localized at the juxtaparanodes of myelinated axons and associates with K+ channels. Neuron. 1999;24:1037–1047. doi: 10.1016/s0896-6273(00)81049-1. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
