

Long-term radiological and pulmonary function abnormalities at 3 years after COVID-19 hospitalisation: a longitudinal cohort study
- PMID: 38387969
- PMCID: PMC11255387
- DOI: 10.1183/13993003.01612-2023
Long-term radiological and pulmonary function abnormalities at 3 years after COVID-19 hospitalisation: a longitudinal cohort study
Abstract
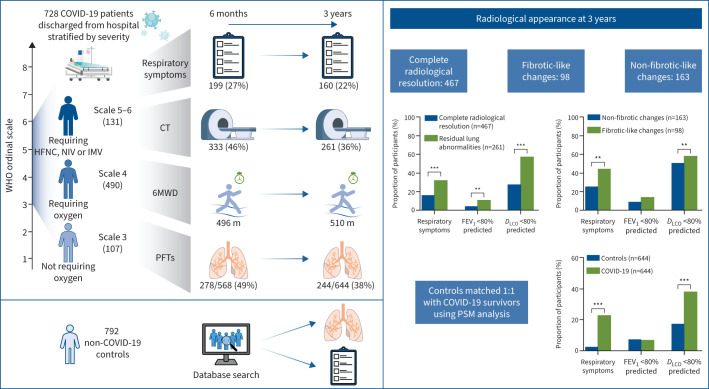
Background: This study aimed to evaluate the longitudinal progression of residual lung abnormalities (ground-glass opacities, reticulation and fibrotic-like changes) and pulmonary function at 3 years following coronavirus disease 2019 (COVID-19).
Methods: This prospective, longitudinal cohort study enrolled COVID-19 survivors who exhibited residual lung abnormalities upon discharge from two hospitals. Follow-up assessments were conducted at 6 months, 12 months, 2 years and 3 years post-discharge, and included pulmonary function tests, 6-min walk distance (6MWD), chest computed tomography (CT) scans and symptom questionnaires. Non-COVID-19 controls were retrospectively recruited for comparative analysis.
Results: 728 COVID-19 survivors and 792 controls were included. From 6 months to 3 years, there was a gradual improvement in reduced diffusing capacity of the lung for carbon monoxide (D LCO <80% predicted: 49% versus 38%; p=0.001), 6MWD (496 versus 510 m; p=0.002) and residual lung abnormalities (46% versus 36%; p<0.001), regardless of disease severity. Patients with residual lung abnormalities at 3 years more commonly had respiratory symptoms (32% versus 16%; p<0.001), lower 6MWD (494 versus 510 m; p=0.003) and abnormal D LCO (57% versus 27%; p<0.001) compared with those with complete resolution. Compared with controls, the proportions of D LCO impairment (38% versus 17%; p<0.001) and respiratory symptoms (23% versus 2.2%; p<0.001) were significantly higher in the matched COVID-19 survivors at the 3-year follow-up.
Conclusions: Most patients exhibited improvement in radiological abnormalities and pulmonary function over time following COVID-19. However, more than a third continued to have persistent lung abnormalities at the 3-year mark, which were associated with respiratory symptoms and reduced diffusion capacity.
Copyright ©The authors 2024.
Conflict of interest statement
Conflict of interest: The authors have no potential conflicts of interest to disclose.
Figures




Comment in
-
Murder, she wrote: a long story on long COVID is being written.Eur Respir J. 2024 Jul 18;64(1):2400916. doi: 10.1183/13993003.00916-2024. Print 2024 Jul. Eur Respir J. 2024. PMID: 39025516 No abstract available.
References
-
- World Health Organization . From emergency response to long-term COVID-19 disease management: sustaining gains made during the COVID-19 pandemic. 2023. www.who.int/publications/i/item/WHO-WHE-SPP-2023.1 Date last accessed: 10 February 2024.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical