

Beyond traditional therapies: a network meta-analysis on the treatment efficacy for chronic phantom limb pain
- PMID: 38388020
- PMCID: PMC12015063
- DOI: 10.1136/rapm-2023-105104
Beyond traditional therapies: a network meta-analysis on the treatment efficacy for chronic phantom limb pain
Abstract
Background: Phantom limb pain (PLP) frequently affects individuals with limb amputations. When PLP evolves into its chronic phase, known as chronic PLP, traditional therapies often fall short in providing sufficient relief. The optimal intervention for chronic PLP remains unclear.
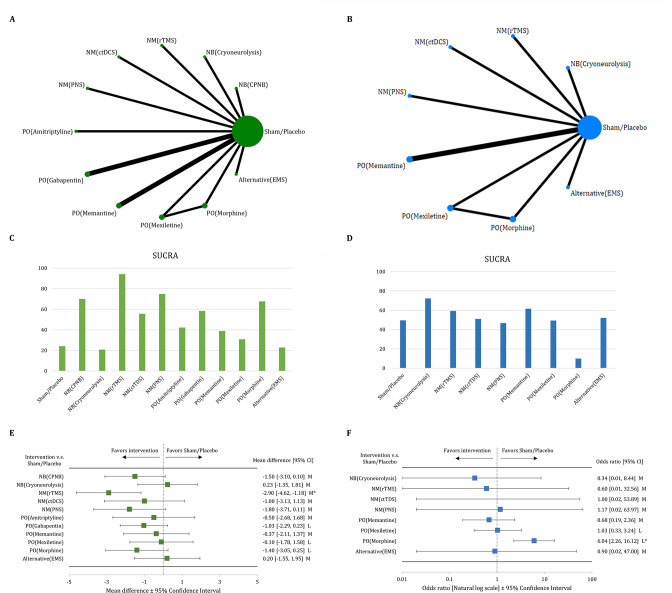
Objective: The objectives of this network meta-analysis (NMA) were to examine the efficacy of different treatments on pain intensity for patients with chronic PLP.
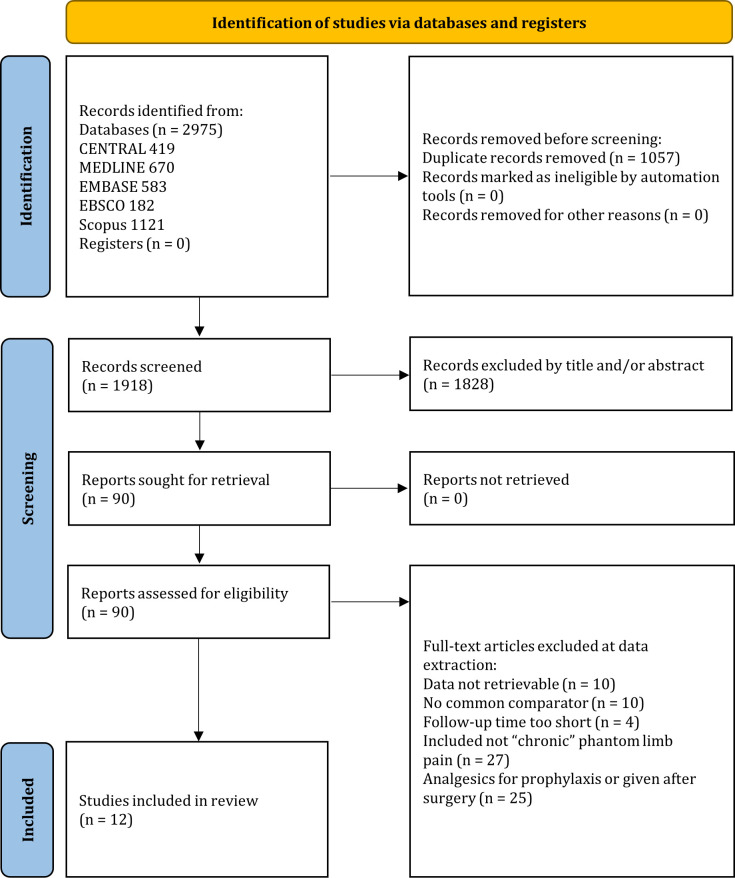
Evidence review: We searched Medline, EMBASE, Cochrane CENTRAL, Scopus, and CINAHL EBSCO, focusing on randomized controlled trials (RCTs) that evaluated interventions such as neuromodulation, neural block, pharmacological methods, and alternative treatments. An NMA was conducted based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. The primary outcome was pain score improvement, and the secondary outcomes were adverse events.
Findings: The NMA, incorporating 12 RCTs, indicated that neuromodulation, specifically repetitive transcranial magnetic stimulation, provided the most substantial pain improvement when compared with placebo/sham groups (mean difference=-2.9 points, 95% CI=-4.62 to -1.18; quality of evidence (QoE): moderate). Pharmacological intervention using morphine was associated with a significant increase in adverse event rate (OR=6.04, 95% CI=2.26 to 16.12; QoE: low).
Conclusions: The NMA suggests that neuromodulation using repetitive transcranial magnetic stimulation may be associated with significantly larger pain improvement for chronic PLP. However, the paucity of studies, varying patient characteristics across each trial, and absence of long-term results underscore the necessity for more comprehensive, large-scale RCTs.
Prospero registration number: CRD42023455949.
Keywords: CHRONIC PAIN; Nerve Block; Pharmacology; analgesia.
© American Society of Regional Anesthesia & Pain Medicine 2025. Re-use permitted under CC BY-NC. No commercial re-use. Published by BMJ Group.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Wiech K, Kiefer R-T, Töpfner S, et al. A placebo-controlled randomized crossover trial of the N-methyl-D-aspartic acid receptor antagonist, memantine, in patients with chronic phantom limb pain. Anesth Analg. 2004;98:408–13. doi: 10.1213/01.ANE.0000096002.53818.BD. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials