

A model-based approach to estimating the prevalence of disease combinations in South Africa
- PMID: 38388163
- PMCID: PMC10884267
- DOI: 10.1136/bmjgh-2023-013376
A model-based approach to estimating the prevalence of disease combinations in South Africa
Abstract
Background: The development of strategies to better detect and manage patients with multiple long-term conditions requires estimates of the most prevalent condition combinations. However, standard meta-analysis tools are not well suited to synthesising heterogeneous multimorbidity data.
Methods: We developed a statistical model to synthesise data on associations between diseases and nationally representative prevalence estimates and applied the model to South Africa. Published and unpublished data were reviewed, and meta-regression analysis was conducted to assess pairwise associations between 10 conditions: arthritis, asthma, chronic obstructive pulmonary disease (COPD), depression, diabetes, HIV, hypertension, ischaemic heart disease (IHD), stroke and tuberculosis. The national prevalence of each condition in individuals aged 15 and older was then independently estimated, and these estimates were integrated with the ORs from the meta-regressions in a statistical model, to estimate the national prevalence of each condition combination.
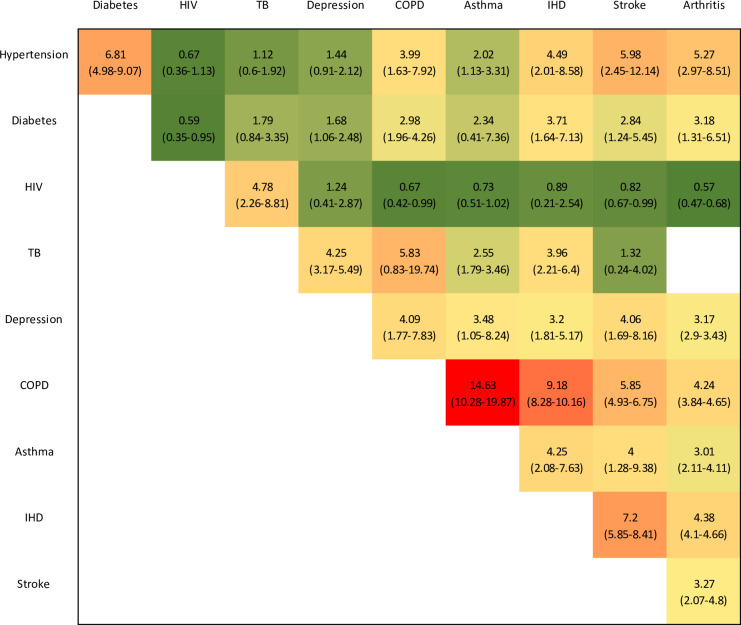
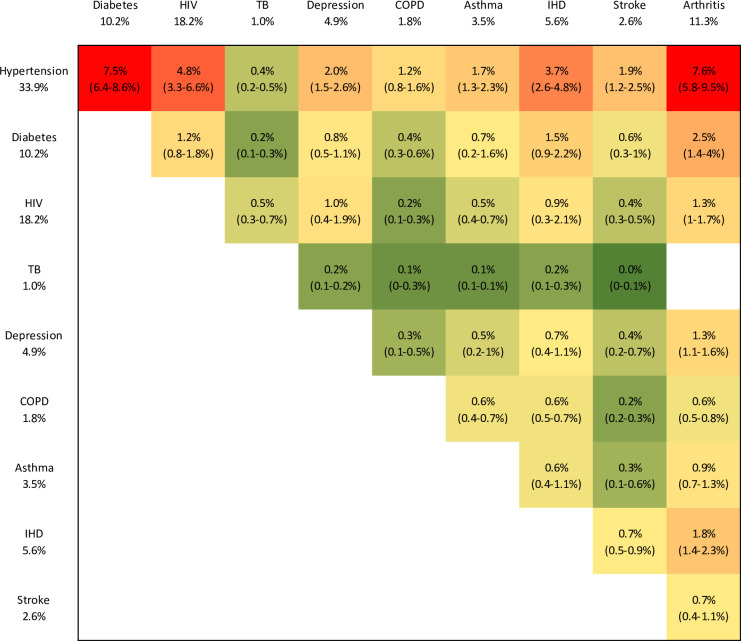
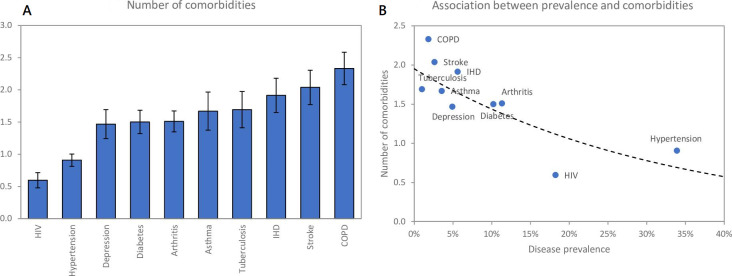
Results: The strongest disease associations in South Africa are between COPD and asthma (OR 14.6, 95% CI 10.3 to 19.9), COPD and IHD (OR 9.2, 95% CI 8.3 to 10.2) and IHD and stroke (OR 7.2, 95% CI 5.9 to 8.4). The most prevalent condition combinations in individuals aged 15+ are hypertension and arthritis (7.6%, 95% CI 5.8% to 9.5%), hypertension and diabetes (7.5%, 95% CI 6.4% to 8.6%) and hypertension and HIV (4.8%, 95% CI 3.3% to 6.6%). The average numbers of comorbidities are greatest in the case of COPD (2.3, 95% CI 2.1 to 2.6), stroke (2.1, 95% CI 1.8 to 2.4) and IHD (1.9, 95% CI 1.6 to 2.2).
Conclusion: South Africa has high levels of HIV, hypertension, diabetes and arthritis, by international standards, and these are reflected in the most prevalent condition combinations. However, less prevalent conditions such as COPD, stroke and IHD contribute disproportionately to the multimorbidity burden, with high rates of comorbidity. This modelling approach can be used in other settings to characterise the most important disease combinations and levels of comorbidity.
Keywords: South Africa; comorbidity; multimorbidity; multiple long-term conditions; non-communicable diseases.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources