

Ethnicity data resource in population-wide health records: completeness, coverage and granularity of diversity
- PMID: 38388690
- PMCID: PMC10883937
- DOI: 10.1038/s41597-024-02958-1
Ethnicity data resource in population-wide health records: completeness, coverage and granularity of diversity
Abstract
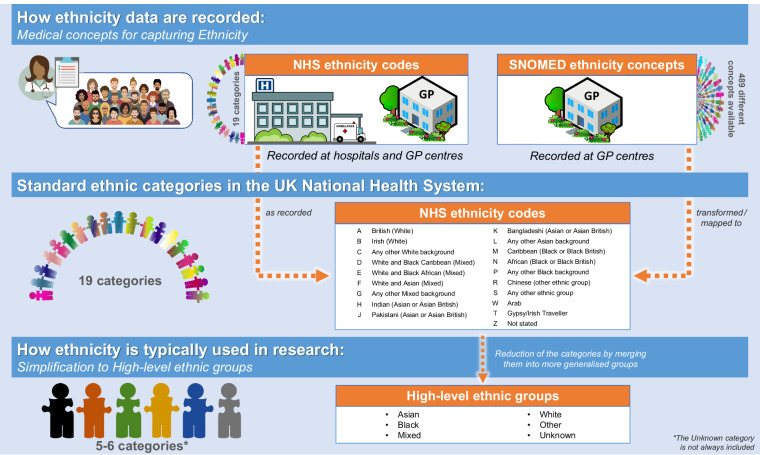
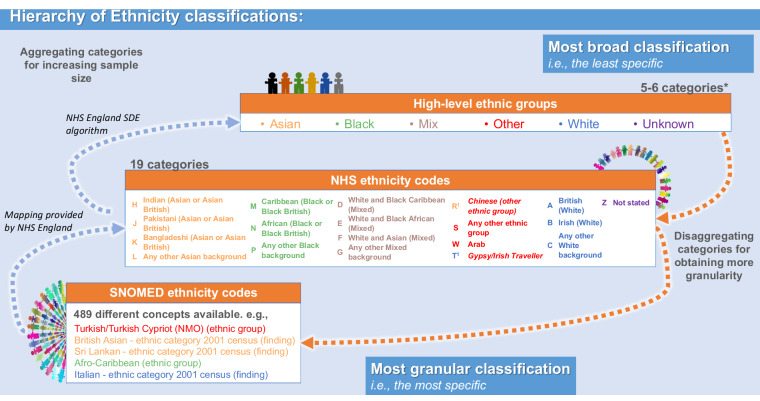
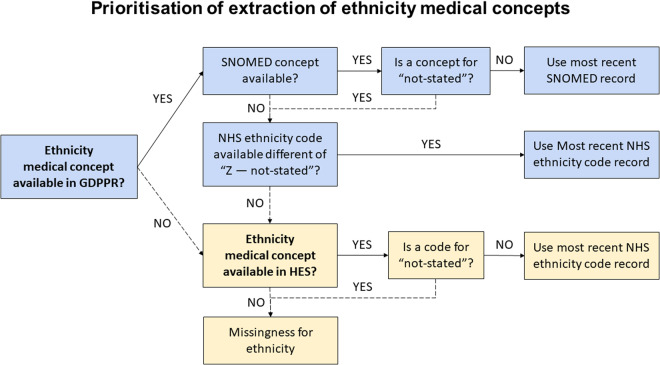
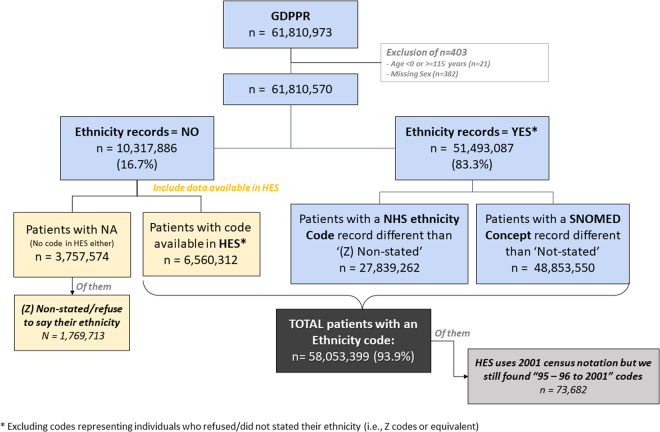
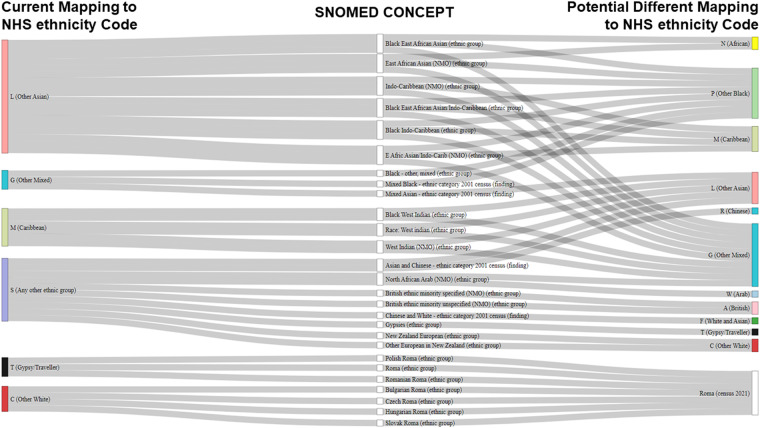
Intersectional social determinants including ethnicity are vital in health research. We curated a population-wide data resource of self-identified ethnicity data from over 60 million individuals in England primary care, linking it to hospital records. We assessed ethnicity data in terms of completeness, consistency, and granularity and found one in ten individuals do not have ethnicity information recorded in primary care. By linking to hospital records, ethnicity data were completed for 94% of individuals. By reconciling SNOMED-CT concepts and census-level categories into a consistent hierarchy, we organised more than 250 ethnicity sub-groups including and beyond "White", "Black", "Asian", "Mixed" and "Other, and found them to be distributed in proportions similar to the general population. This large observational dataset presents an algorithmic hierarchy to represent self-identified ethnicity data collected across heterogeneous healthcare settings. Accurate and easily accessible ethnicity data can lead to a better understanding of population diversity, which is important to address disparities and influence policy recommendations that can translate into better, fairer health for all.
© 2024. The Author(s).
Conflict of interest statement
AA is supported by Health Data Research UK (HDR-9006), which receives its funding from the UK Medical Research Council (MRC, grant MR/V028367/1); and Administrative Data Research UK, which is funded by the ESRC (grant ES/S007393/1). SD is supported by: BigData@Heart Consortium, funded by the Innovative Medicines Initiative-2 Joint Undertaking under grant agreement 116074, The British Heart Foundation Data Science Centre (grant No SP/19/3/34678, awarded to Health Data Research (HDR) UK), NIHR Biomedical Research Centre at University College London (UCL) Hospital NHS Trust, the NIHR-UKRI CONVALESCENCE study, BHF Accelerator Award (AA/18/6/24223). CT is supported by a UCL UKRI Centre for Doctoral Training in AI-enabled Healthcare studentship (EP/S021612/1), MRC Clinical Top-Up and a studentship from the NIHR Biomedical Research Centre at University College London Hospital NHS Trust. KK is the director of Centre for Ethnic Health Research, and trustee of South Asian Health Foundation. SK has received research grant funding from the UKRI and Alan Turing Institute for this work, and from Amgen and UCB Biopharma, and Bill & Melinda Gates Foundation outside of this work. DPA’s research group has received grant/s from Amgen, Chiesi-Taylor, Lilly, Janssen, Novartis, and UCB Biopharma. His research group has received consultancy fees from Astra Zeneca and UCB Biopharma. Amgen, Astellas, Janssen, Synapse Management Partners and UCB Biopharma have funded or supported training programmes organised by SK and DPA’s department. The remaining authors have nothing to declare.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
