

Artificial intelligence support in MR imaging of incidental renal masses: an early health technology assessment
- PMID: 38388721
- PMCID: PMC11364579
- DOI: 10.1007/s00330-024-10643-5
Artificial intelligence support in MR imaging of incidental renal masses: an early health technology assessment
Abstract
Objective: This study analyzes the potential cost-effectiveness of integrating an artificial intelligence (AI)-assisted system into the differentiation of incidental renal lesions as benign or malignant on MR images during follow-up.
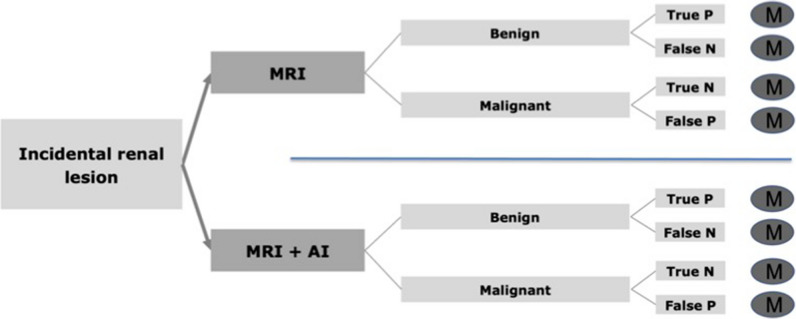
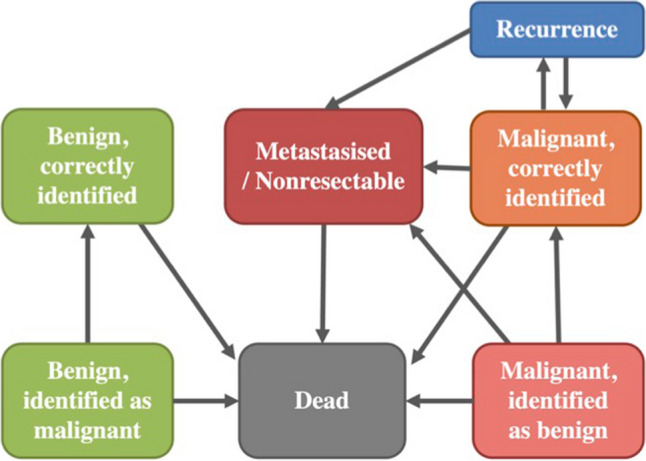
Materials and methods: For estimation of quality-adjusted life years (QALYs) and lifetime costs, a decision model was created, including the MRI strategy and MRI + AI strategy. Model input parameters were derived from recent literature. Willingness to pay (WTP) was set to $100,000/QALY. Costs of $0 for the AI were assumed in the base-case scenario. Model uncertainty and costs of the AI system were assessed using deterministic and probabilistic sensitivity analysis.
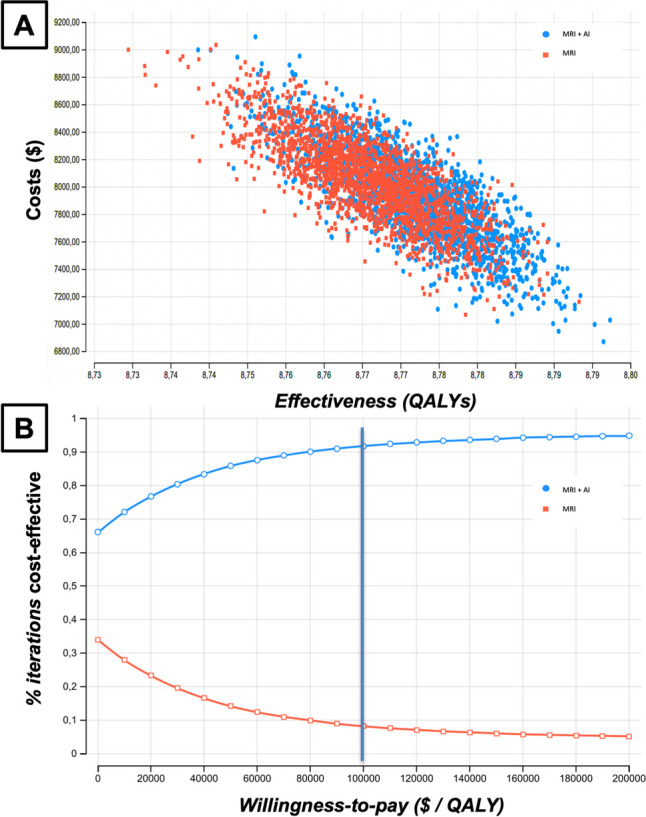
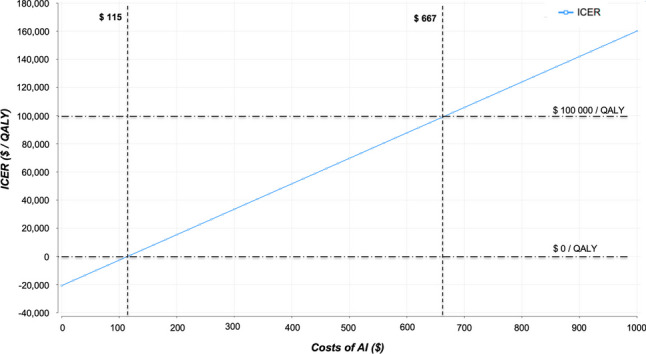
Results: Average total costs were at $8054 for the MRI strategy and $7939 for additional use of an AI-based algorithm. The model yielded a cumulative effectiveness of 8.76 QALYs for the MRI strategy and of 8.77 for the MRI + AI strategy. The economically dominant strategy was MRI + AI. Deterministic and probabilistic sensitivity analysis showed high robustness of the model with the incremental cost-effectiveness ratio (ICER), which represents the incremental cost associated with one additional QALY gained, remaining below the WTP for variation of the input parameters. If increasing costs for the algorithm, the ICER of $0/QALY was exceeded at $115, and the defined WTP was exceeded at $667 for the use of the AI.
Conclusions: This analysis, rooted in assumptions, suggests that the additional use of an AI-based algorithm may be a potentially cost-effective alternative in the differentiation of incidental renal lesions using MRI and needs to be confirmed in the future.
Clinical relevance statement: These results hint at AI's the potential impact on diagnosing renal masses. While the current study urges careful interpretation, ongoing research is essential to confirm and seamlessly integrate AI into clinical practice, ensuring its efficacy in routine diagnostics.
Key points: • This is a model-based study using data from literature where AI has been applied in the diagnostic workup of incidental renal lesions. • MRI + AI has the potential to be a cost-effective alternative in the differentiation of incidental renal lesions. • The additional use of AI can reduce costs in the diagnostic workup of incidental renal lesions.
Keywords: Artificial intelligence; Cost-effectiveness analysis; Incidental findings; Kidney; MRI.
© 2024. The Author(s).
Conflict of interest statement
JR is a member of the European Radiology Advisory Editorial Board. He has not taken part in the review or selection process of this article
Figures

Comment in
-
Early health technology assessment: the value of valuing AI applications.Eur Radiol. 2024 Sep;34(9):5854-5855. doi: 10.1007/s00330-024-10749-w. Epub 2024 Apr 20. Eur Radiol. 2024. PMID: 38642110 No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
