

A case report of carcinoma of the papilla of Vater associated with a hyperplasia-dysplasia-carcinoma sequence by pancreaticobiliary maljunction
- PMID: 38389074
- PMCID: PMC10882841
- DOI: 10.1186/s12957-024-03347-z
A case report of carcinoma of the papilla of Vater associated with a hyperplasia-dysplasia-carcinoma sequence by pancreaticobiliary maljunction
Abstract
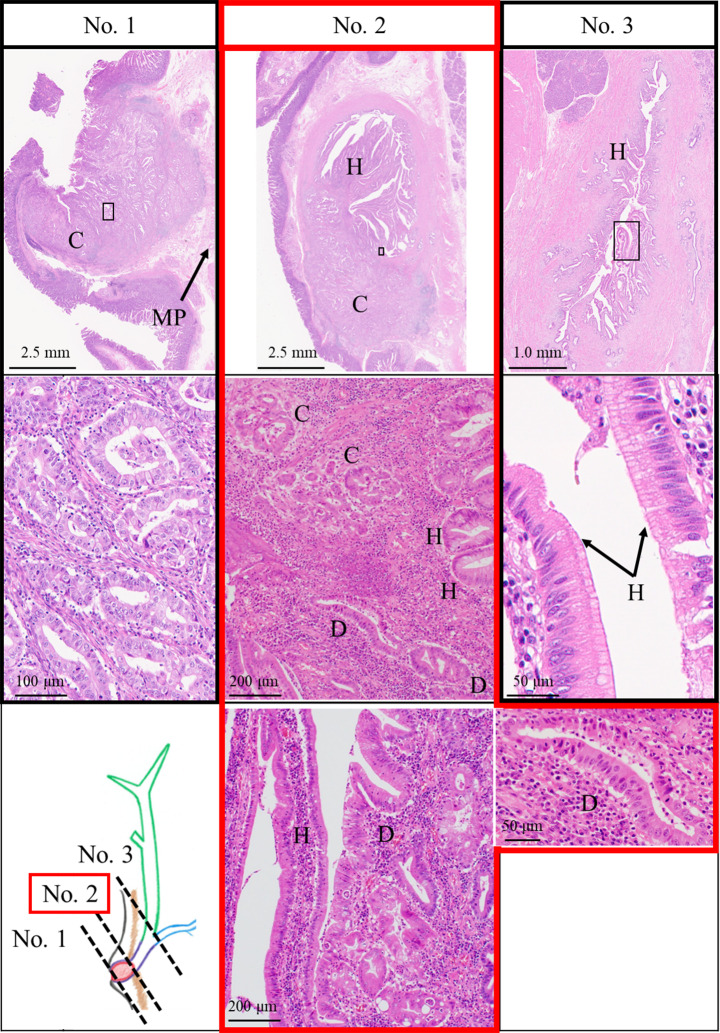
Background: Pancreaticobiliary maljunction (PBM) is a known risk factor for biliary tract cancer. However, its association with carcinoma of the papilla of Vater (PVca) remains unknown. We report a case with PVca that was thought to be caused by the hyperplasia-dysplasia-carcinoma sequence, which is considered a mechanism underlying PBM-induced biliary tract cancer.
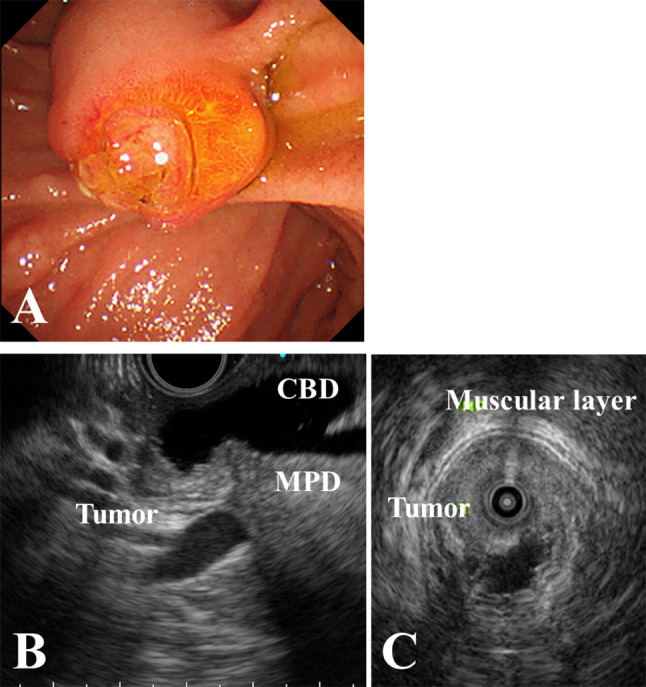
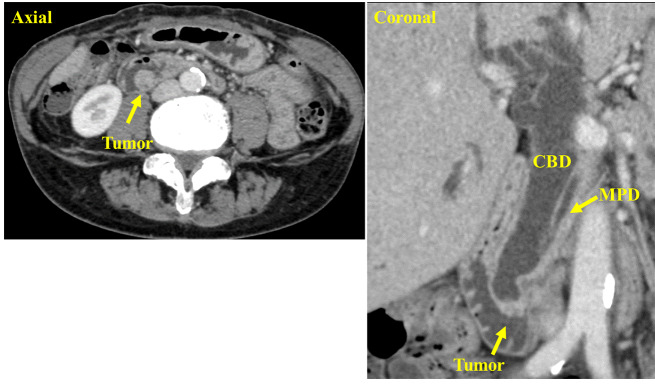
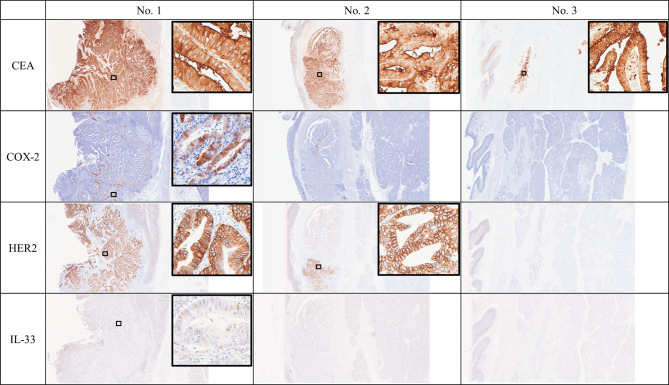
Case presentation: A 70-year-old woman presented with white stool and had a history of cholecystectomy for the diagnosis of a non-dilated biliary tract with PBM. Esophagogastroduodenoscopy revealed a tumor in the papilla of Vater, and PVca was histologically proven by biopsy. We finally diagnosed her with PVca concurrent with non-biliary dilated PBM (cT1aN0M0, cStage IA, according to the Union for International Cancer Control, 8th edition), and subsequently performed subtotal stomach-preserving pancreaticoduodenectomy. Pathological findings of the resected specimen revealed no adenomas and dysplastic and hyperplastic mucosae in the common channel slightly upstream of the main tumor, suggesting a PBM related carcinogenic pathway with hyperplasia-dysplasia-carcinoma sequence. Immunostaining revealed positivity for CEA. CK7 positivity, CK20 negativity, and MUC2 negativity indicated that this PVca was of the pancreatobiliary type. Genetic mutations were exclusively detected in tumors and not in normal tissues, and bile ducts from formalin-fixed paraffin-embedded samples included mutated-ERBB2 (Mutant allele frequency, 81.95%). Moreover, of the cell-free deoxyribonucleic acid (cfDNA) extracted from liquid biopsy mutated-ERBB2 was considered the circulating-tumor deoxyribonucleic acid (ctDNA) of this tumor.
Conclusions: Herein, we report the first case of PVca with PBM potentially caused by a "hyperplasia-dysplasia-carcinoma sequence" detected using immunostaining and next-generation sequencing. Careful follow-up is required if pancreaticobiliary reflux persists, considering the possible development of PVca.
Keywords: Carcinoma of the papilla of Vater; Dysplasia; ERBB2; Formalin-fixed paraffin-embedded; Hyperplasia; Liquid biopsy; Next-generation sequencing; Pancreaticobiliary maljunction; cfDNA; ctDNA.
© 2024. The Author(s).
Conflict of interest statement
The following authors declare that they have no competing interests: TK, YK, KW, SKL, MI, MN, KK, TM, TK, YK, DK, TS, AM, YK, YM, HN, and IT.
Figures

Similar articles
-
Biliary carcinogenesis in pancreaticobiliary maljunction.J Gastroenterol. 2017 Feb;52(2):158-163. doi: 10.1007/s00535-016-1268-z. Epub 2016 Oct 4. J Gastroenterol. 2017. PMID: 27704265 Review.
-
Pancreaticobiliary maljunction and carcinogenesis to biliary and pancreatic malignancy.Langenbecks Arch Surg. 2009 Jan;394(1):159-69. doi: 10.1007/s00423-008-0336-0. Epub 2008 May 24. Langenbecks Arch Surg. 2009. PMID: 18500533 Review.
-
Intracholecystic papillary neoplasm arising in a patient with pancreaticobiliary maljunction: a case report.World J Surg Oncol. 2020 Nov 9;18(1):292. doi: 10.1186/s12957-020-02072-7. World J Surg Oncol. 2020. PMID: 33168026 Free PMC article.
-
Multiple Cancers of the Biliary Tract and Pancreatic Duct after Cholecystectomy for Gallbladder Cancer in a Patient with Pancreaticobiliary Maljunction.Intern Med. 2016;55(2):141-6. doi: 10.2169/internalmedicine.55.4706. Epub 2016 Jan 15. Intern Med. 2016. PMID: 26781013
-
Carcinoma of the Papilla of Vater after Diversion Operation for Pancreaticobiliary Maljunction.Case Rep Gastroenterol. 2017 May 17;11(2):265-270. doi: 10.1159/000462967. eCollection 2017 May-Aug. Case Rep Gastroenterol. 2017. PMID: 28626371 Free PMC article.
References
-
- The Japanese study group on pancreaticobiliary Maljunction (JSPBM) The Committee of JSPBM for Diagnostic Criteria. Diagnostic criteria of pancreaticobiliary maljunction. J Hepato-Bil Pancreat Surg. 1994;1:219–21. doi: 10.1007/BF02391070. - DOI
-
- Morine Y, Mori H, Utsunomiya T, Imura S, Ikemoto T, Ishibashi H, et al. Epidemiology and clinical features of pancreaticobiliary Maljunction. J Jpn Biliary Assoc. 2011;25:133–40.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
