

Preoperative evaluation to determine the difficulty of No. 6 lymphadenectomy in laparoscopic gastrectomy
- PMID: 38389108
- PMCID: PMC10885599
- DOI: 10.1186/s12893-024-02349-8
Preoperative evaluation to determine the difficulty of No. 6 lymphadenectomy in laparoscopic gastrectomy
Abstract
Background: Laparoscopic gastrectomy (LG) requires a long learning curve because of the complicated surgical procedures. Infrapyloric (No. 6) lymph node dissection (LND) is one of the difficult procedures in LG, especially for trainees. This study investigated the impact of the prediction of the difficulty of No. 6 LND.
Methods: We retrospectively reviewed the preoperative computed tomography (CT) images and individual operative video records of 57 patients who underwent LG with No. 6 LND to define and predict the No. 6 LND difficulty. To evaluate whether prediction of the difficulty of No. 6 LND could improve surgical outcomes, 48 patients who underwent laparoscopic distal gastrectomy were assessed (30 patients without prediction by a qualified surgeon and 18 patients with prediction by a trainee).
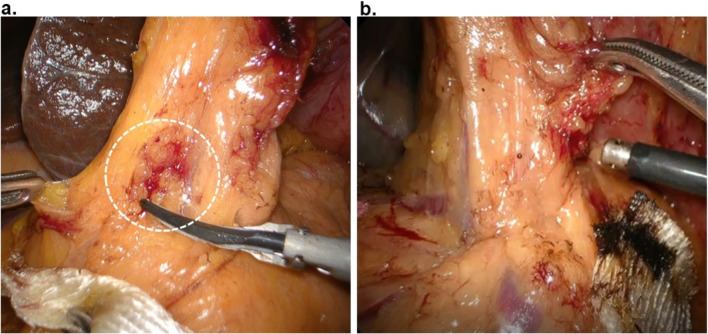
Results: The anatomical characteristic that LND required > 2 cm of dissection along the right gastroepiploic vein was defined as difficulty of No. 6 LND. Of the 57 LG patients, difficulty was identified intraoperatively in 21 patients (36.8%). Among the several evaluated anatomical parameters, the length between the right gastroepiploic vein and the right gastroepiploic artery in the maximum intensity projection in contrast-enhanced CT images was significantly correlated with the intraoperative difficulty of No. 6 LND (p < 0.0001). Surgical outcomes, namely intraoperative minor bleeding, postoperative pancreatic fistula, and drain amylase concentration were not significantly different between LG performed by a trainee with prediction compared with that by a specialist without prediction.
Conclusions: Preoperative evaluation of the difficulty of No. 6 LND is useful for trainees, to improve surgical outcomes.
Keywords: Gastric cancer; Laparoscopic gastrectomy; No. 6 LND; Pancreatic fistula; Prediction; Trainee.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


Similar articles
-
Outermost layer-oriented medial approach for infrapyloric nodal dissection in laparoscopic distal gastrectomy.Surg Endosc. 2018 Apr;32(4):2137-2148. doi: 10.1007/s00464-018-6111-6. Epub 2018 Feb 15. Surg Endosc. 2018. PMID: 29450630
-
[Preliminary experience of dual-port laparoscopic distal gastrectomy for gastric cancer].Zhonghua Wei Chang Wai Ke Za Zhi. 2019 Jan 25;22(1):35-42. Zhonghua Wei Chang Wai Ke Za Zhi. 2019. PMID: 30703792 Chinese.
-
Factors affecting the quality of laparoscopic D2 lymph node dissection for gastric cancer: a cohort study from two randomized controlled trials.Int J Surg. 2023 May 1;109(5):1249-1256. doi: 10.1097/JS9.0000000000000290. Int J Surg. 2023. PMID: 37026819 Free PMC article.
-
Radical Lymph Node Dissection Along the Proximal Splenic Artery During Laparoscopic Gastrectomy for Gastric Cancer Using the Left Lateral Approach.Ann Surg Oncol. 2017 Sep;24(9):2727. doi: 10.1245/s10434-017-5877-4. Epub 2017 May 15. Ann Surg Oncol. 2017. PMID: 28508144
-
Laparoscopic-assisted versus open distal gastrectomy with D2 lymph node resection for advanced gastric cancer: effect of learning curve on short-term outcomes. a meta-analysis.J Laparoendosc Adv Surg Tech A. 2014 Mar;24(3):139-50. doi: 10.1089/lap.2013.0481. J Laparoendosc Adv Surg Tech A. 2014. PMID: 24625347 Review.
References
-
- Inaki N, Etoh T, Ohyama T, Uchiyama K, Katada N, Koeda K, Yoshida K, Takagane A, Kojima K, Sakuramoto S, et al. A multi-institutional, prospective, phase II feasibility study of Laparoscopy-assisted distal gastrectomy with D2 lymph node dissection for locally advanced gastric Cancer (JLSSG0901) World J Surg. 2015;39(11):2734–41. doi: 10.1007/s00268-015-3160-z. - DOI - PubMed
-
- Hiki N, Fukunaga T, Yamaguchi T, Nunobe S, Tokunaga M, Ohyama S, Seto Y, Yoshiba H, Nohara K, Inoue H, et al. The benefits of standardizing the operative procedure for the assistant in laparoscopy-assisted gastrectomy for gastric cancer. Langenbeck’s Archives Surg. 2008;393(6):963–71. doi: 10.1007/s00423-008-0374-7. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
